Download to read offline

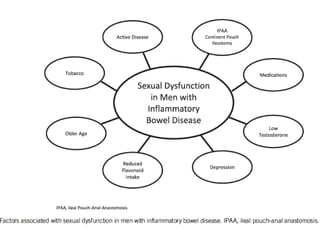
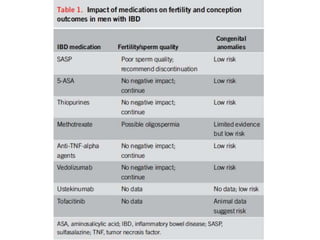
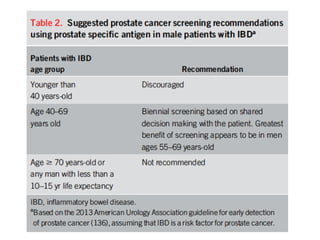
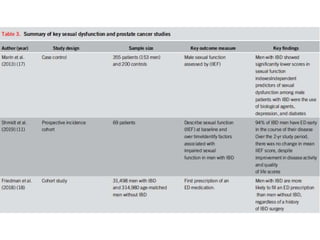
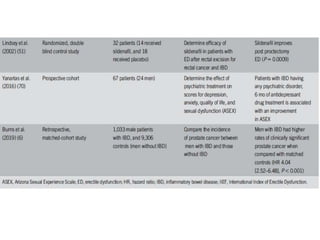
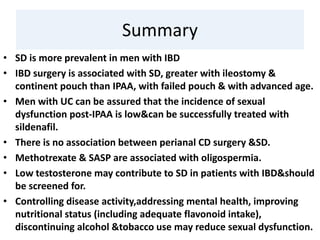

- Sexual dysfunction and infertility are more prevalent in men with IBD compared to the general population. - Depression is the most consistent negative predictive factor of sexual function among men with IBD. - Sulfasalazine can reversibly reduce male fertility, so it is recommended to discontinue 3-4 months prior to conception. Most other IBD medications do not significantly impact fertility. - Men with IBD have an increased risk of prostate cancer and prostate cancer screening guidelines for higher risk patients should be followed.