Download as PDF, PPTX


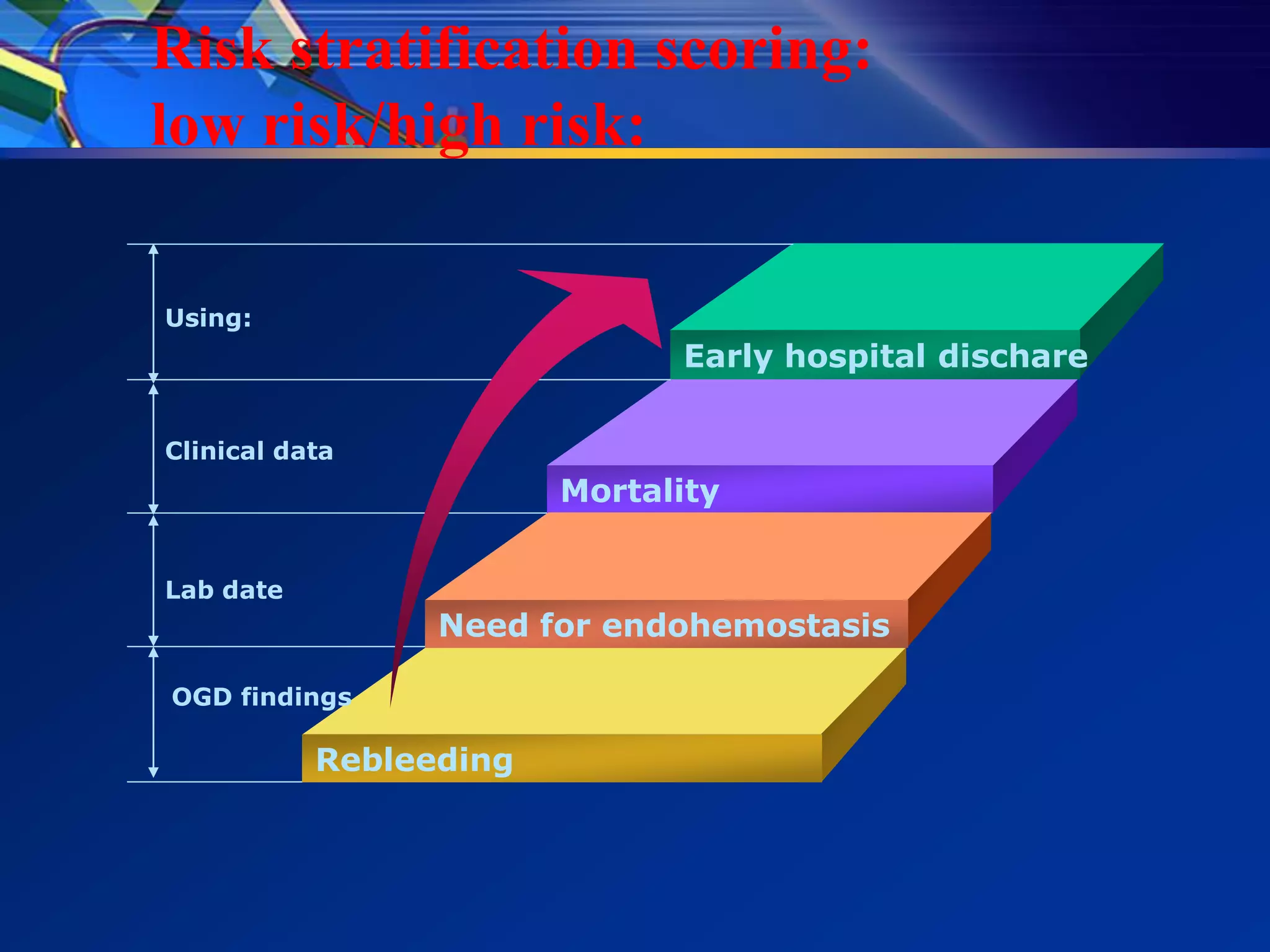
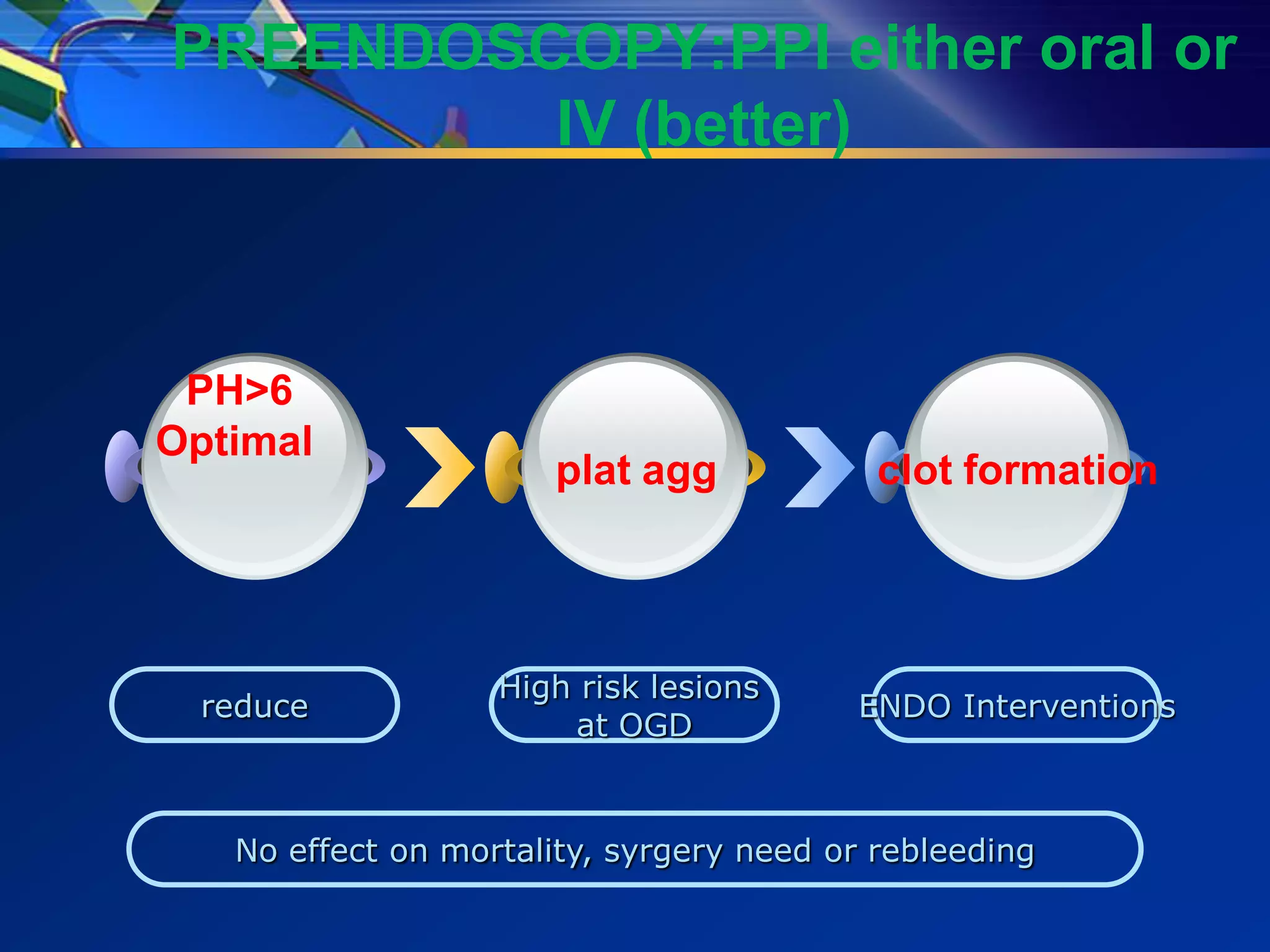
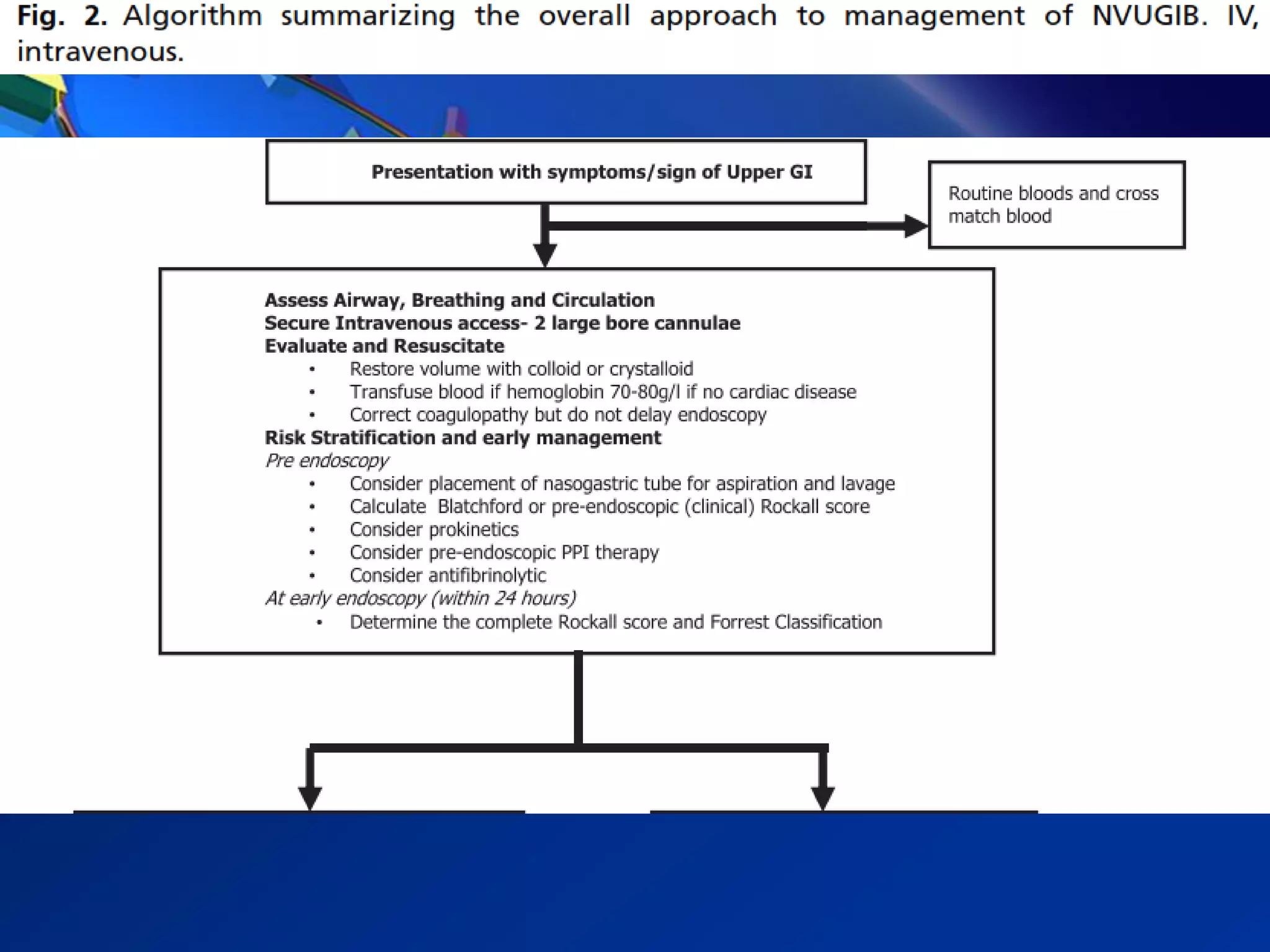
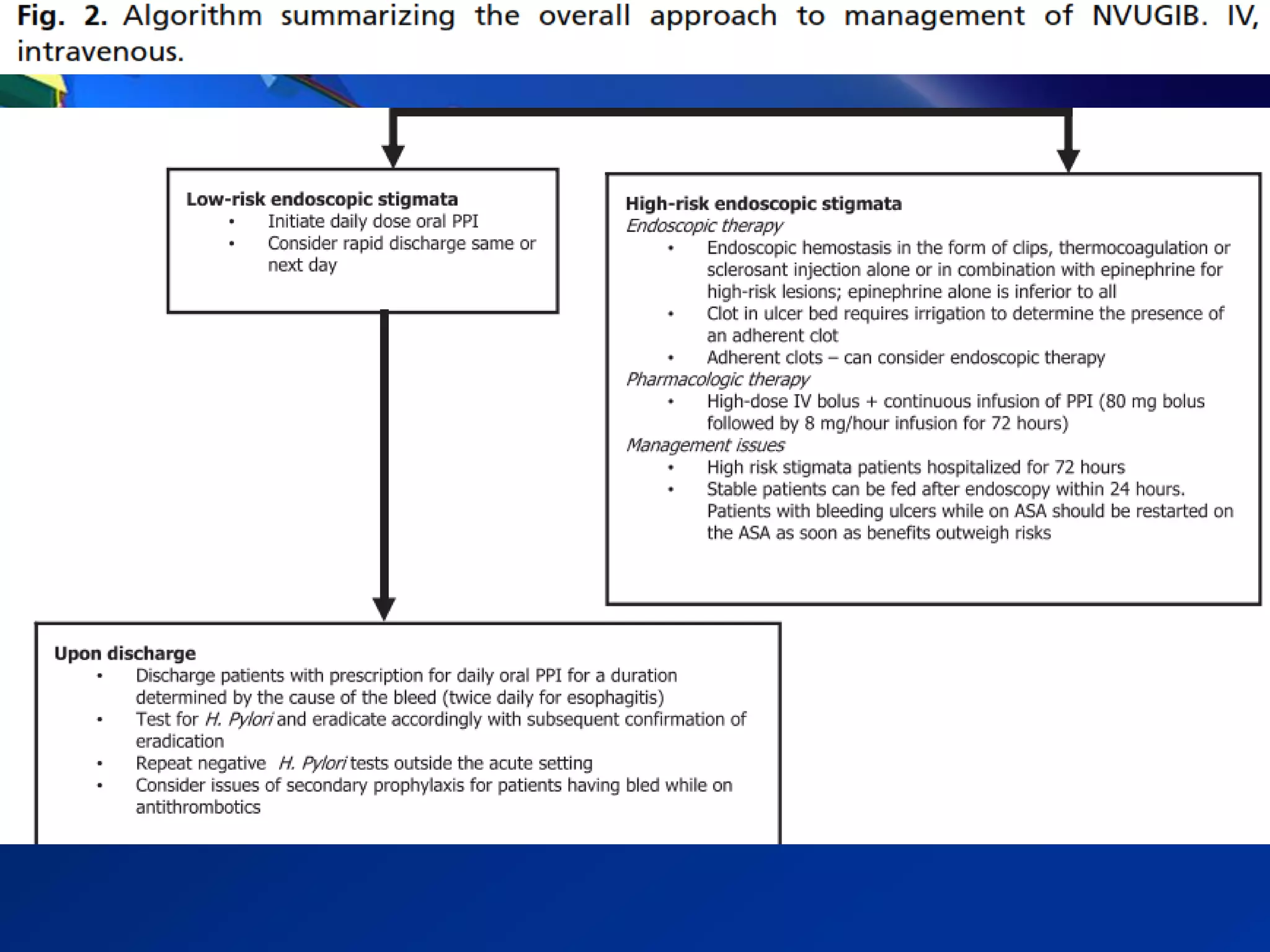
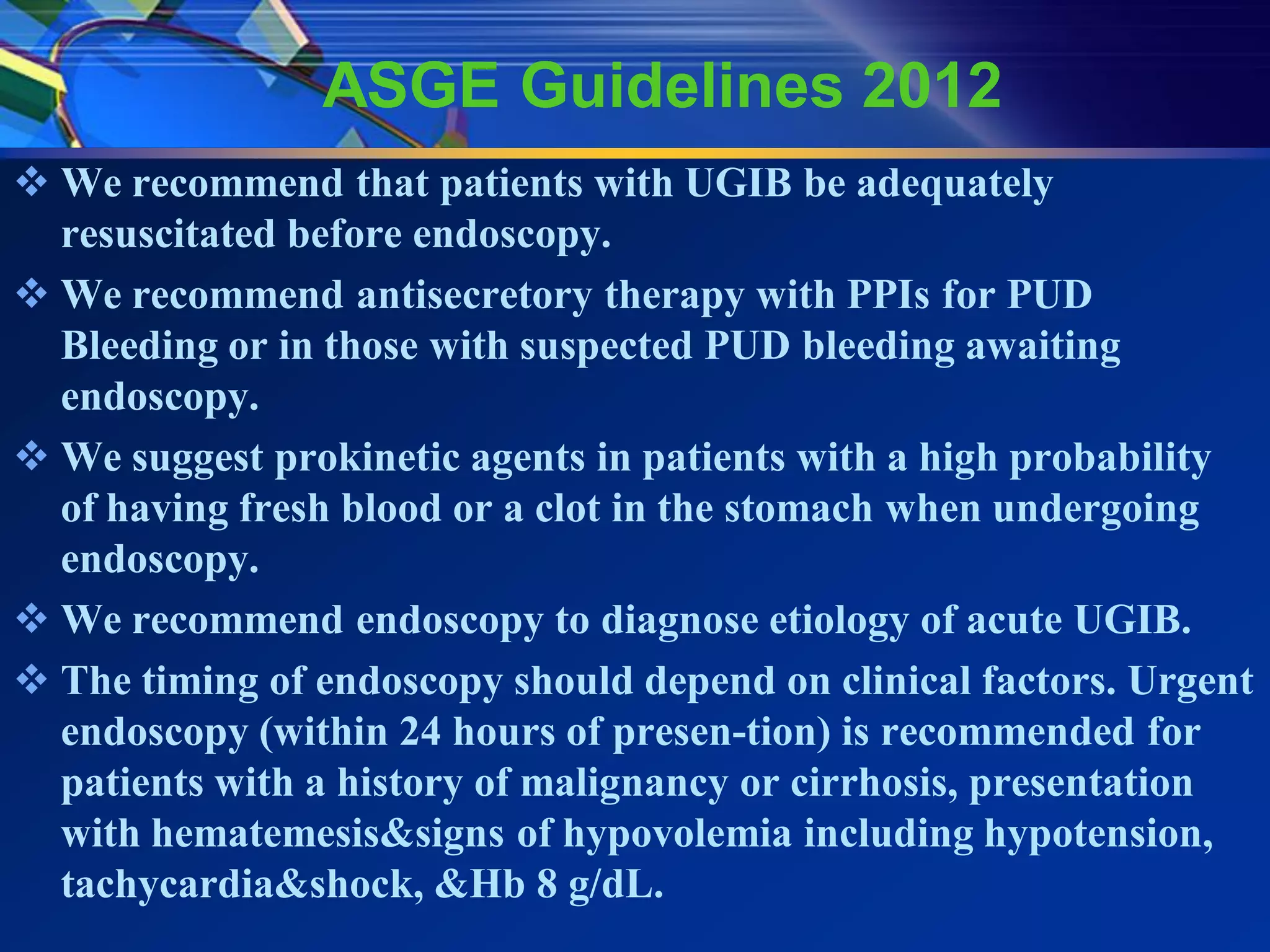
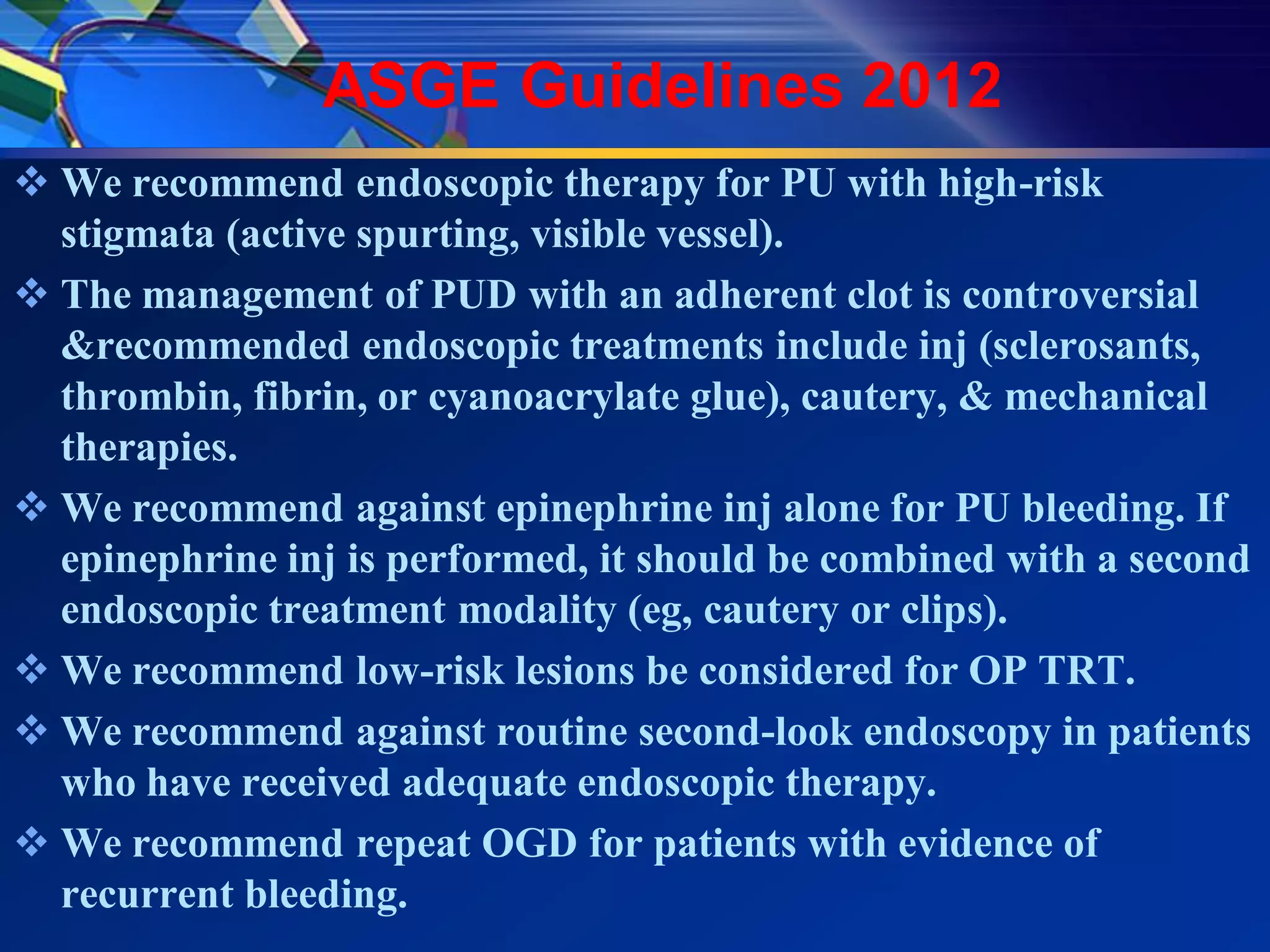
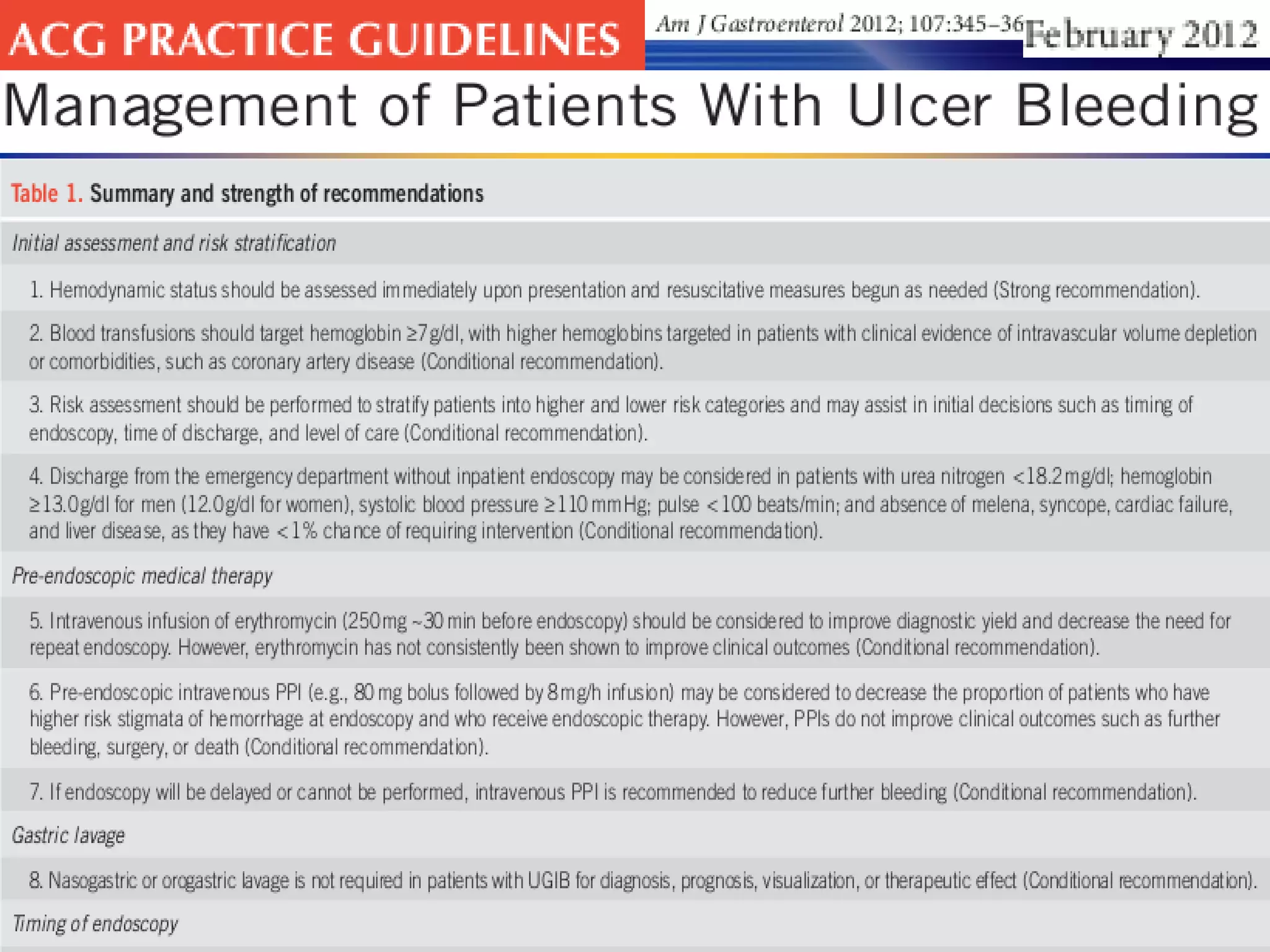

1) Gastrointestinal bleeding can occur in the upper or lower GI tract. UGIB is more common and has a higher mortality rate than LGIB. 2) Common causes of UGIB include peptic ulcer disease, erosive gastritis, and esophageal tears. Management involves resuscitation, risk stratification, early endoscopy within 24 hours, and endoscopic therapy for high-risk lesions. 3) Guidelines recommend adequate resuscitation, antisecretory therapy for suspected peptic ulcer bleeding, and endoscopic treatment combining epinephrine injection with a second modality for high-risk ulcers to achieve hemostasis.