Downloaded 13 times
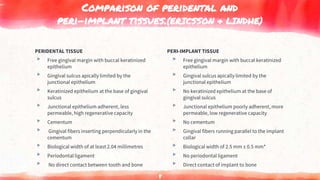
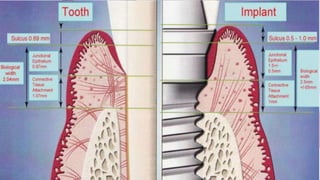
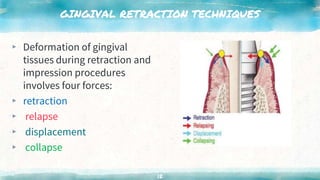








This document discusses various techniques for gingival retraction during dental impressions for implants. It begins with introductions to implant dentistry and the need for gingival retraction during impressions. The document then compares the peridental and peri-implant tissues. It reviews the requirements and goals of gingival retraction as well as various retraction techniques including mechanical, chemomechanical, and surgical approaches. The document also discusses some recent advancements in gingival retraction techniques such as Expasyl, Magic Foamcord, and Gingitrac which aim to provide retraction with less trauma to tissues.



































































