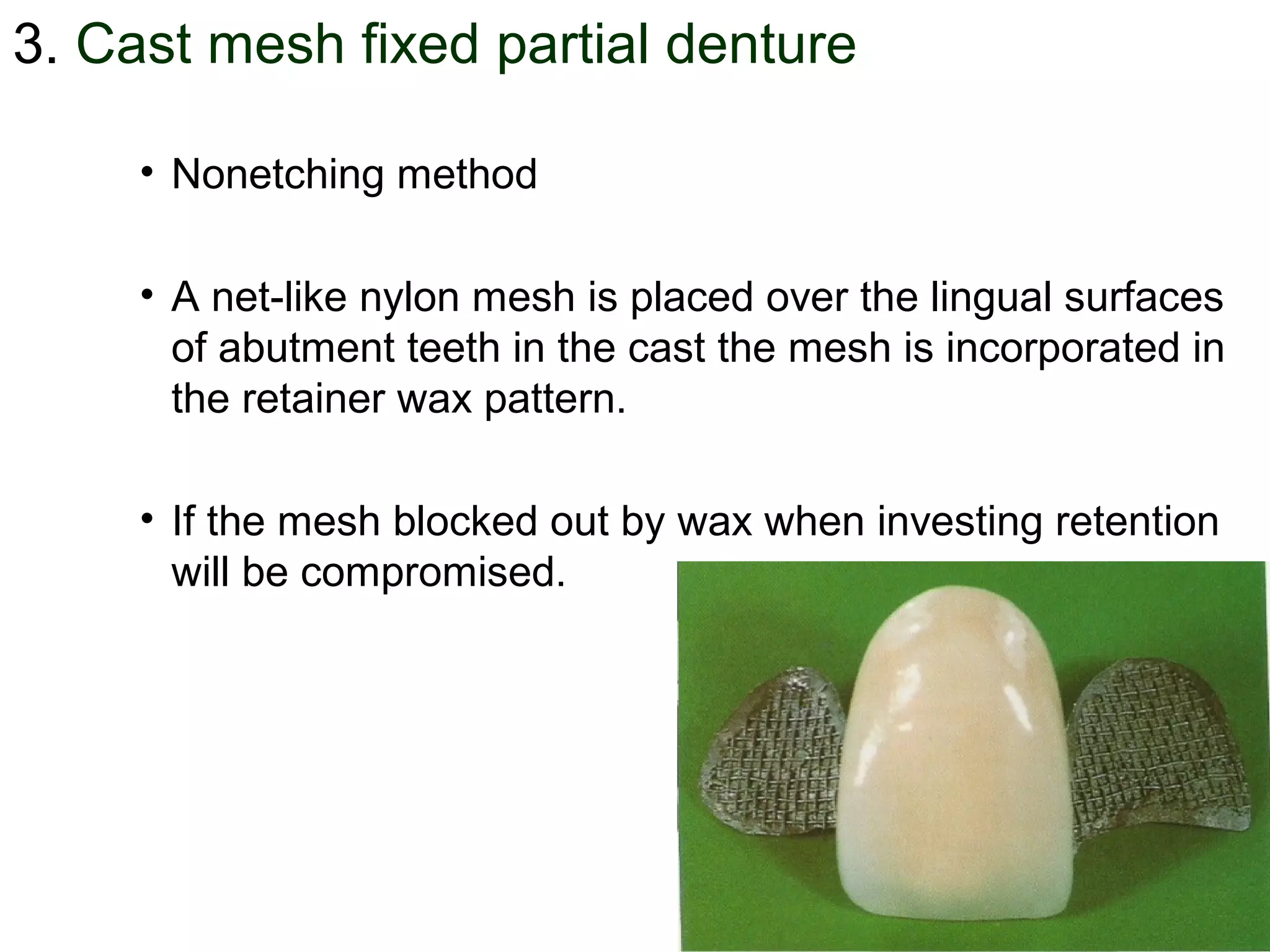
This document discusses resin-bonded fixed partial dentures (FPDs). It introduces resin-bonded FPDs as a way to minimize destruction of sound tooth structure compared to conventional FPDs. Resin-bonded FPDs have a metal framework that is bonded to abutment teeth with resin cement after minimal tooth preparation. Several types of resin-bonded FPD designs are described, including Rochette, Maryland, cast mesh, and Virginia bridges. The techniques, advantages, disadvantages, indications, and contraindications of resin-bonded FPDs are outlined. Tooth preparation for resin-bonded FPDs involves minimal axial reduction and guide planes on proximal surfaces.