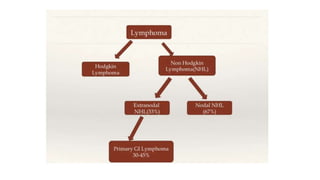
- Gastrointestinal lymphomas originate from lymphoid cells in the gastrointestinal tract. The two main types are non-Hodgkin lymphoma and Hodgkin lymphoma.
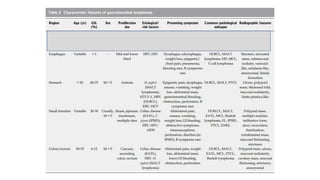
- Primary gastrointestinal lymphomas are rare, accounting for about 1-4% of gastrointestinal malignancies. The stomach is the most commonly involved site. Histopathologically, almost 90% are B cell lymphomas.
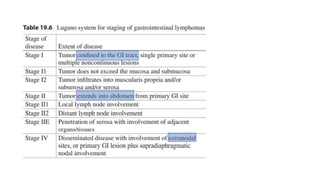
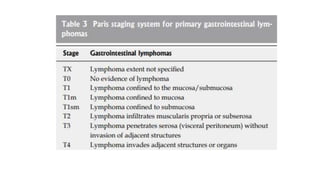
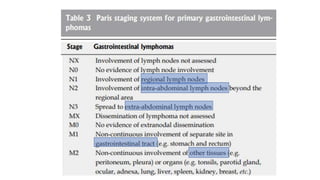
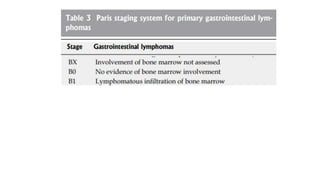
- Proper staging of primary gastrointestinal lymphomas includes physical exam, endoscopic ultrasound, CT scan, PET scan, and bone marrow biopsy according to the Lugano or Paris staging systems. Treatment involves chemotherapy, radiation, surgery or a combination depending on the histological subtype and extent of disease.


![• Multiple regimens used in other B-cell lymphomas have demonstrated activity in
FL, including
o CHOP and
o CVP (cyclophosphamide, vincristine, and prednisone) as well as
o Fludarabine based regimens (fludarabine and cyclophosphamide [FC];
fludarabine, cyclophosphamide, and mitoxantrone [FCM]),
o Chlorambucil, and
o Bendamustine in combination with rituximab](https://image.slidesharecdn.com/gastrointestinallymphoma-230401173047-af149267/85/Gastrointestinal-Lymphoma-pptx-128-320.jpg)