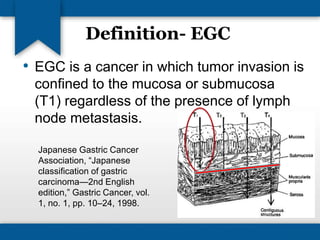
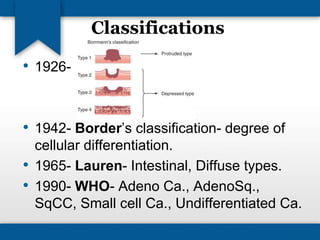
Early gastric cancer (EGC) is defined as tumors confined to the mucosa or submucosa, with good prognosis and high 5-year survival rates. Increasing detection rates in countries like Japan and Korea contrast with much lower rates in the U.S. Various risk factors, diagnostic methods, and treatments are discussed, including minimally invasive endoscopic approaches, with future possibilities such as laparoscopy-assisted techniques.