Downloaded 22 times

![IMMEDIATE POST-NATAL
MANAGEMENT
Resuscitation;Airway,Breathing,Circulation.
The rate of infusion of lactated ringers solution
at 2-3 times the normal maintenance should be
guided by the clinical condition of the patient
determined by the pulse rate,MAP,and urine
output, electrolytes, Hct, and base deficit
Catheterization to monitor urinary output and
to provide more space for bowel reduction.
Antibiotics; Vitamin K ;. [Blood glucose]
monitoring www.mednotez.eazzymedicine.co
m](https://image.slidesharecdn.com/abdominalwalldefectspesantation-190613123951/85/Abdominal-wall-defects-pesantation-25-320.jpg)

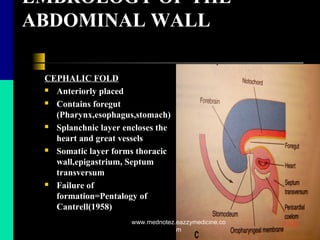
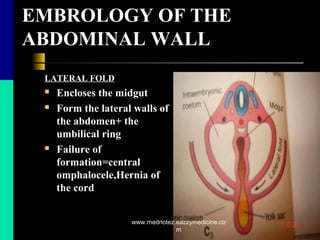
![INTRODUCTION
ERYTHROPOIETIN (EPO)
Growth factor produced by the kidney in
response to anemia.
Found in human milk and has functional Epo
receptors in fetal and postnatal small
intestines[7].
Binds to enterocytes and stimulates small
intestinal growth by increasing length, villous
surface area, villi height, and ileal crypt depth
[8].
Protects neurons against ischaemia-induced
cell death. Acts as an angiogenic growth factor
for intestinal mesentery microvascular
endothelial cells [9,10].
www.mednotez.eazzymedicine.co
m](https://image.slidesharecdn.com/abdominalwalldefectspesantation-190613123951/85/Abdominal-wall-defects-pesantation-41-320.jpg)
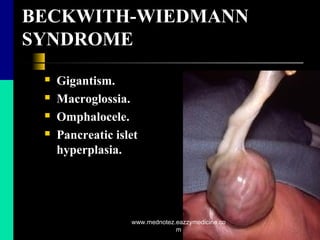
![MATERIALS AND METHODS
All experimental procedures were approved by
Ethical Committee of the Dr. Behcet Uz
Children’s Hospital.
Thirteen-day-old fertilized chick eggs were
incubated at 37.5C in 80% humidity.
Operative procedures for all groups were
performed on the 13th day of incubation, using
previously published methods [11].
www.mednotez.eazzymedicine.co
m](https://image.slidesharecdn.com/abdominalwalldefectspesantation-190613123951/85/Abdominal-wall-defects-pesantation-43-320.jpg)
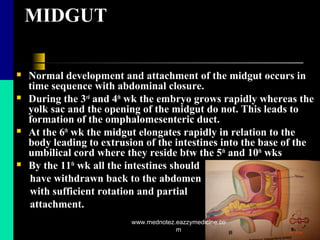
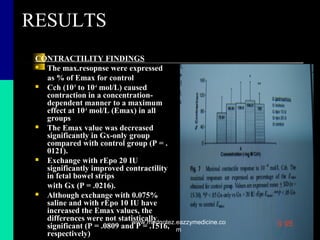
![MATERIALS AND METHODS
CONTRACTILITY STUDIES
Cumulative carbachol concentration response
curve was constructed for each sample.
The response was expressed as a percentage of
the maximum Cch-evoked contraction (Emax)
in the control group.[fig.7]
Maximal response to Cch in the Gx-only group
was compared with the other groups using
Mann-Whitney U test. P <.05 was considered
significant.
www.mednotez.eazzymedicine.co
m](https://image.slidesharecdn.com/abdominalwalldefectspesantation-190613123951/85/Abdominal-wall-defects-pesantation-49-320.jpg)
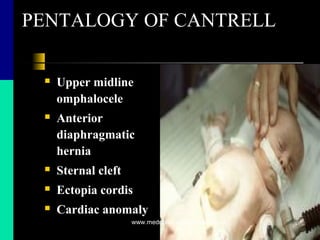
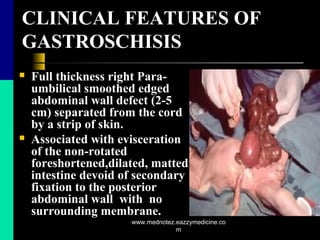
![DISCUSSION
Significant postoperative morbidity still occurs as a
consequence of bowel damage in utero despite prenatal
diagnosis and immediate appropriate neonatal
care[12].
Previous studies [13,14 ] have reported amnioinfusion
to decrease morphological bowel damage in
experimental animal studies as well as in human Gx.
Though controversy still exists on pathogenesis and
treatment of the intestinal malfunction .
The present study demonstrated that intraamniotic
rEpo administration restores, in a dose dependent
manner, both morphological damage and intestinal
dysfunction associated with Gx.
www.mednotez.eazzymedicine.co
m](https://image.slidesharecdn.com/abdominalwalldefectspesantation-190613123951/85/Abdominal-wall-defects-pesantation-57-320.jpg)
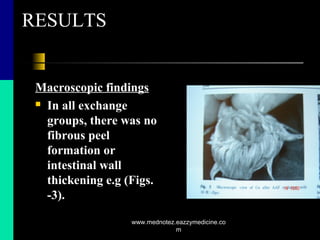
![DISCUSSION
Exposure of the intestines to AAF in Gx-only
group resulted in bowel wall thickening,
fibrous peel and adhesions as described in
previous reports [16].
Amnioinfusion with either only physiological
saline or rEpo+ saline, =>normal appearing
intestines.=> that AAF exchange decreases the
concentration of harmful chemicals responsible
for intestinal morphological damage, as
previously reported in other clinical and
experimental studies [17].
www.mednotez.eazzymedicine.co
m](https://image.slidesharecdn.com/abdominalwalldefectspesantation-190613123951/85/Abdominal-wall-defects-pesantation-58-320.jpg)
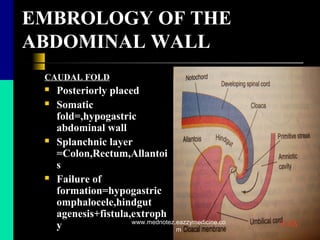
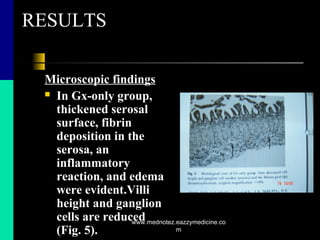
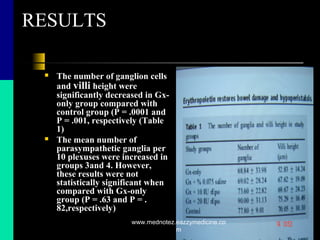
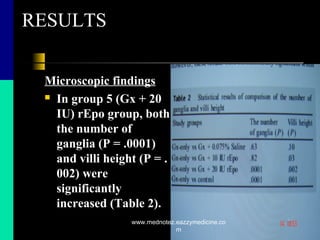
![DISCUSSION
In the study, ganglia were morphologically normal in
all groups but there was a significant decrease in the
number of ganglia in Gx-only group.
AAF exchange with physiological saline did not
increased the number of ganglion cells but a dose-
dependent increase in the number of ganglia was found
after AAF exchange with rEpo.
This could be attributed to the fact that rEpo
decreases apoptotic death of neuronal cells and
enterocytes [21]and also acts like anti-inflammatory
agents[9].
In the study, bowel contractility and villi height were
significantly lower in Gx-only group than normal.
www.mednotez.eazzymedicine.co
m](https://image.slidesharecdn.com/abdominalwalldefectspesantation-190613123951/85/Abdominal-wall-defects-pesantation-59-320.jpg)
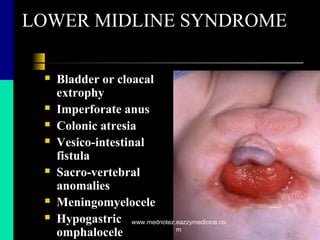
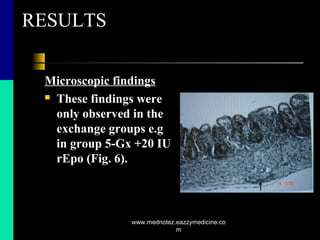
![DISCUSSION
Physiological saline exchange had no significant effect
on either bowel contractility or villi height. In contrast,
AAF exchange with rEpo significantly improved
contractility in a dose-dependent manner; in addition,
histological examination of the bowel mucosa showed
longer villi in both rEpo-treated groups.
This had been shown in previous rat studies, in which
rEpo significantly increased intestinal length and the
absorptive surface of the microvilli, primarily by
increasing the villi length [8]. It is also an angiogenic
growth factor[10].
www.mednotez.eazzymedicine.co
m](https://image.slidesharecdn.com/abdominalwalldefectspesantation-190613123951/85/Abdominal-wall-defects-pesantation-60-320.jpg)
![DISCUSSION
The results suggested that intraamniotic rEpo
administration in Gx acts not only as a trophic factor
but also as a prokinetic agent on a variety of
nonhematopoietic cell types, including enterocytes,
endothelial cells, smooth muscle cells, and neuronal
cells; cell types that are present in the developing bowel
[24].
In conclusion, the data constituted a basis for
examining the effectiveness and appropriate dose of
rEpo in further studies for treatment of all aspects of
intestinal malfunction in human Gx.
www.mednotez.eazzymedicine.co
m](https://image.slidesharecdn.com/abdominalwalldefectspesantation-190613123951/85/Abdominal-wall-defects-pesantation-61-320.jpg)

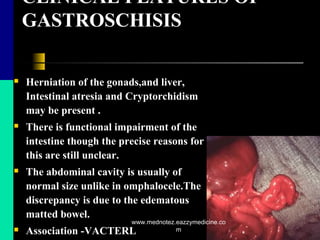
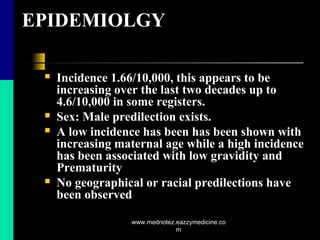
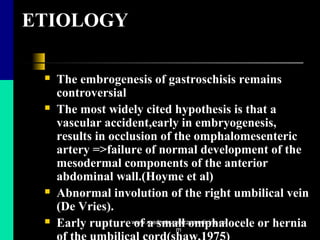
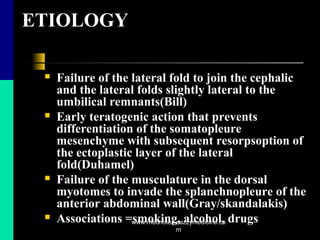
The document provides a comprehensive overview of gastroschisis, including its historical background, embryology, clinical features, epidemiology, etiology, and management. It discusses the pathophysiology related to intestinal dysfunction, prenatal management techniques, surgical interventions, and postoperative care. Furthermore, it highlights the relevant studies regarding the effects of erythropoietin on intestinal health in cases of gastroschisis.







































![Neonatal nursing care for GZIT[Autosaved].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/ambayenntwoassigmentautosaved-231228091237-bb9a1ff0-thumbnail.jpg?width=640&height=640&fit=bounds)



























