Download as ODP, PPTX




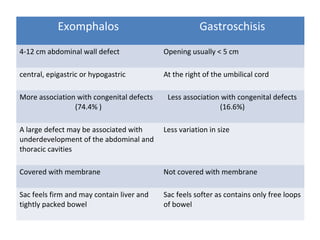









This document discusses anterior abdominal wall defects including exomphalos and gastroschisis. Exomphalos is a congenital abnormality where abdominal contents herniate into the umbilical cord through the umbilical ring and are covered by a membrane. Gastroschisis is a defect of the abdominal wall to the right of the umbilical cord without a covering membrane. The document outlines the epidemiology, presentation, associated diseases, investigations and management of both conditions. It also discusses complications and notes that prognosis has improved over time due to advances in care but significant morbidity can still occur.























































































