Downloaded 73 times
















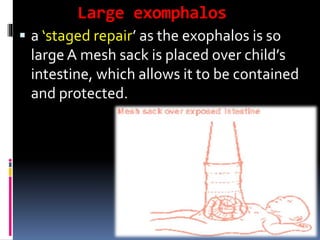






This document defines and describes congenital umbilical hernias and omphaloceles. It explains that an omphalocele is a weakness in the abdominal wall that allows abdominal contents like the bowel and liver to protrude outside the abdomen. There are two types - minor and major - depending on the size of the defect and contents. Treatment for a minor omphalocele involves primary repair to return the intestines to the abdomen, while a major one requires a staged repair using a mesh sack. Outcomes depend on factors like prematurity and other malformations. Ultrasound during pregnancy can often detect an omphalocele.









































































