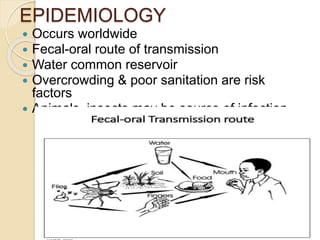
Gastroenteritis is the inflammation of the gastrointestinal tract leading to diarrhea, abdominal cramps, and nausea, and is commonly transmitted via the fecal-oral route. It can be caused by various pathogens including viruses, bacteria, and parasites, with rotavirus being the most prevalent in children. Treatment focuses on rehydration, with oral or intravenous solutions recommended, while antibiotics are selectively used depending on the causative agent.
![ETIOLOGY
Etiologies include bacteria, viruses,
parasites, toxins, and drugs. (eg, metals,
plant substances).
Viruses
Four categories of viruses cause most
gastroenteritis:
rotavirus and calicivirus
(predominantly the norovirus [formerly
Norwalk virus]) cause the majority of viral
gastroenteritis, followed by astrovirus
and enteric adenovirus.](https://image.slidesharecdn.com/gastroenteritis1-180914092425/85/Gastroenteritis-Pharmacotherapy-8-320.jpg)