Downloaded 310 times




![Clinical guideline [CG99]
Published date: May 2010
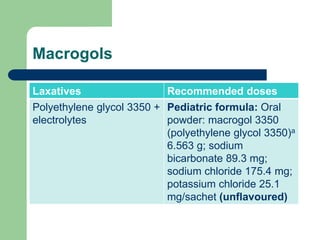
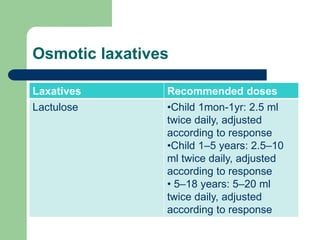
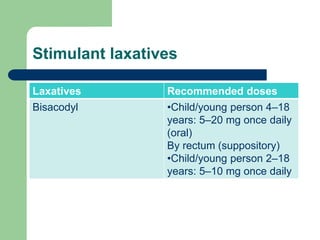
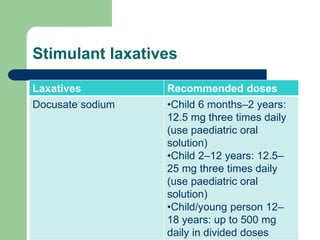
Recommended laxative
doses](https://image.slidesharecdn.com/constipationfinal-170404063011/85/Constipation-31-320.jpg)
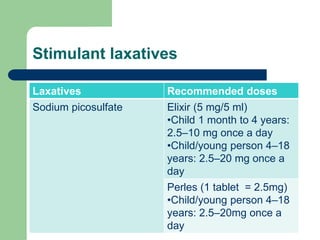


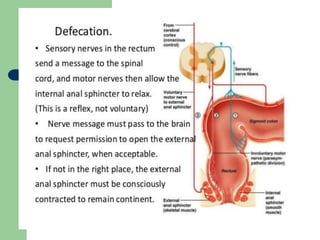
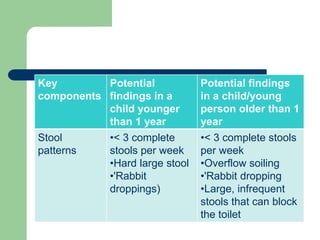
This document defines constipation and provides details about its causes, symptoms, diagnosis and treatment. It begins by defining constipation as difficulty or delay in defecation for at least 2 weeks, and discusses other related terms. It then covers the causes of constipation including functional, organic, dietary and drug-related factors. The key components of diagnosing constipation through history and physical examination are outlined. Rome III diagnostic criteria for children and adults are presented. Finally, the document discusses approaches to treatment including lifestyle changes, bulk-forming laxatives, stimulant laxatives and biofeedback training.


















































































