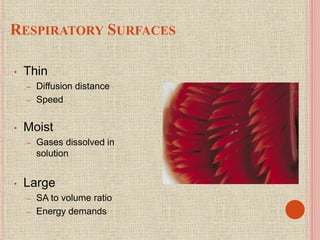
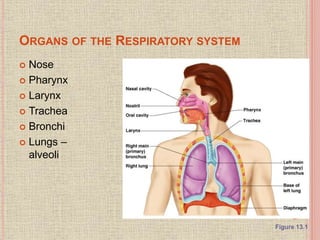
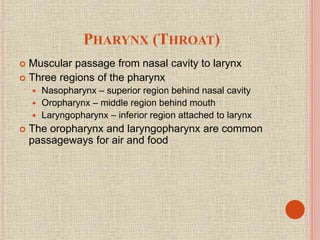
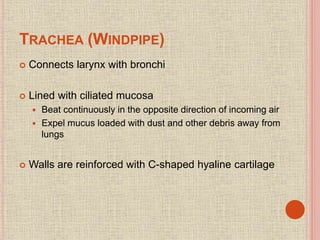
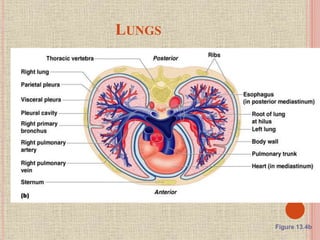
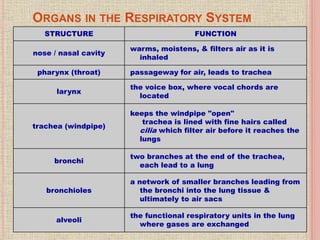
The document discusses the human respiratory system and gas exchange. It describes the major organs involved including the nose, pharynx, larynx, trachea, bronchi, and lungs. It explains the processes of pulmonary ventilation including inspiration and expiration. It discusses oxygen and carbon dioxide transport in the blood and partial pressures of gases in the body. It also covers common respiratory disorders like asthma, pneumonia, and emphysema.