Download as PDF, PPTX



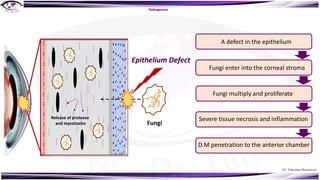



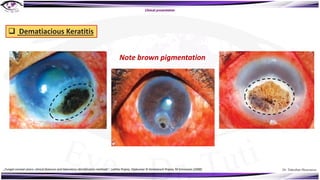
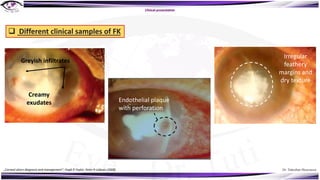
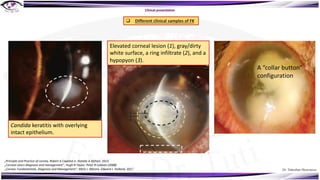
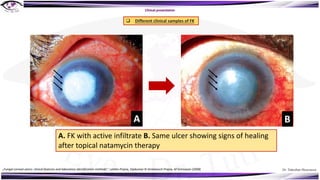

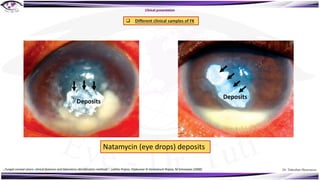
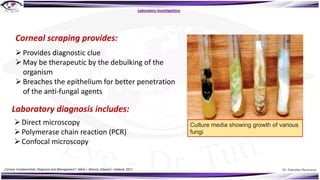


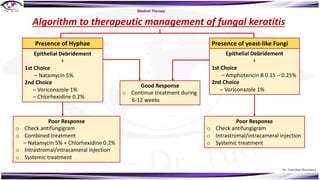





Fungal keratitis is a major cause of eye morbidity and blindness, particularly affecting male outdoor workers in developing countries. It presents with symptoms such as increasing pain, vision loss, and specific signs like feathery margins and satellite lesions, often requiring both medical and surgical interventions. Medical management primarily involves topical antifungals like natamycin and amphotericin B, alongside systemic support, though therapy is complicated by the lack of standard guidelines.



















































































