Corneal Ulcer
Corneal Ulceris defined as discontinuation in normal
epithelium surface of cornea associated with necrosis of
the surrounding corneal tissue.(1)
NOTE: Corneal ulcer refers to tissue excavation associated with an epithelial defect ,
usually with infiltration and necrosis; whereas Corneal Keratitis refers to presence of
tissue inflammation with or without epithelial defect(corneal oedema, cellular
infiltration and ciliary congestion)
1.Khurana, A. K. (2014). Comprehensive Ophthalmology 7E (7th ed.).
3.
Pathogenesis of aCorneal Ulcer (2)
Stromal melting is preceded by a corneal epithelial defect.
Corneal ulcers occur due to the host cellular and immunologic responses to the
offending agent which may be bacterial,viral,fungal or protozoal organism
Polymorphonuclear cells released in response to corneal insult secretes various lytic
enzymes such as collagenases, elastases and cathepsin causing destruction of cornea.
2.Sharma, N., & Vajpayee, R. B. (2008). Corneal ulcer- diagnosis & management. Jaypee Brothers Medi
cal Publishers (P) Ltd.
Stages of CornealUlcer (3)
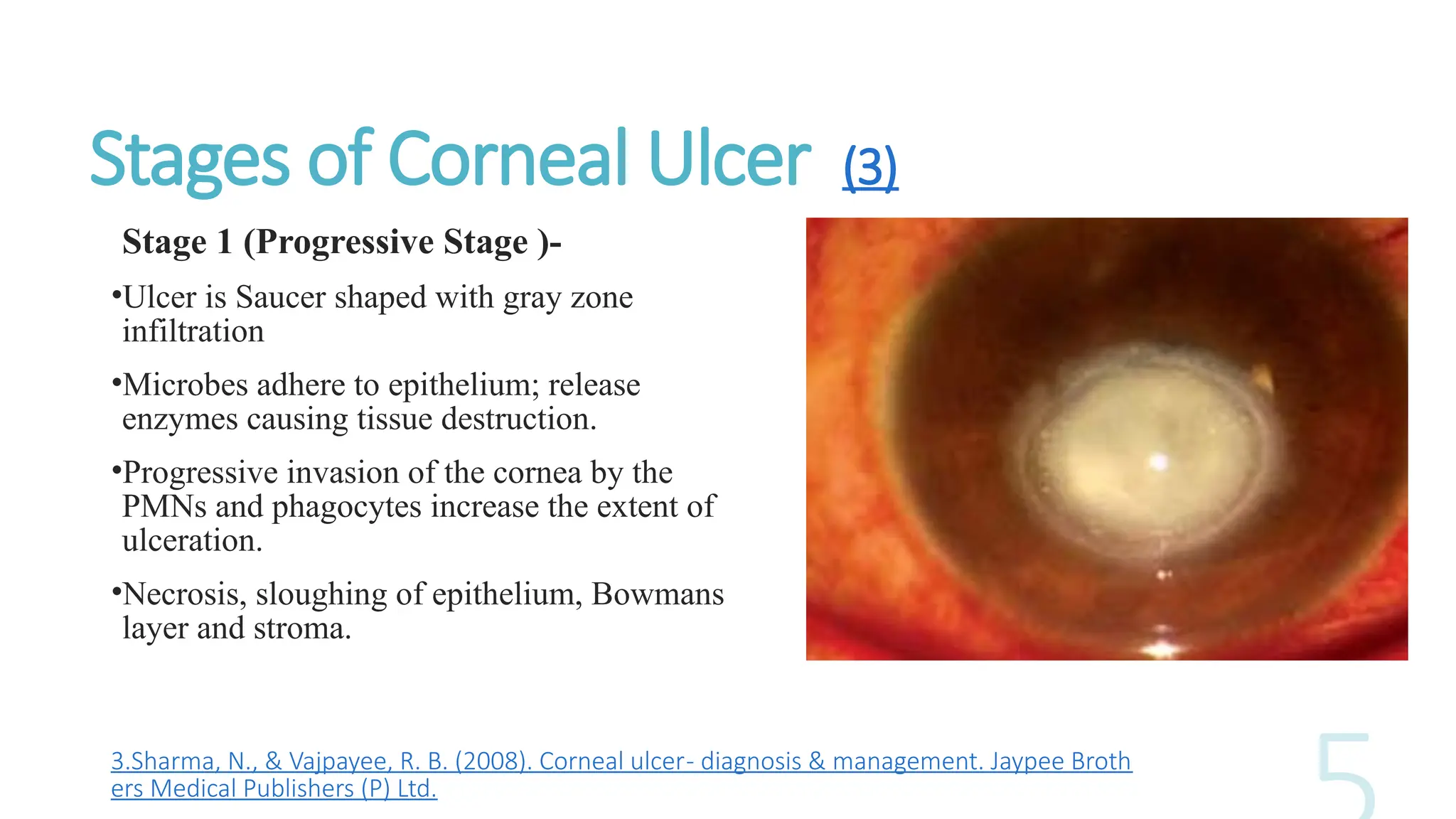
Stage 1 (Progressive Stage )-
•Ulcer is Saucer shaped with gray zone
infiltration
•Microbes adhere to epithelium; release
enzymes causing tissue destruction.
•Progressive invasion of the cornea by the
PMNs and phagocytes increase the extent of
ulceration.
•Necrosis, sloughing of epithelium, Bowmans
layer and stroma.
3.Sharma, N., & Vajpayee, R. B. (2008). Corneal ulcer- diagnosis & management. Jaypee Broth
ers Medical Publishers (P) Ltd.
6.
Stage 2- Regressivestage
•Natural host defense mechanisms(humoral antibody response and cell mediated
response) & antimicrobial treatment.
•Line of demarcation around the ulcer ; margins and floor become smooth and
transparent.
•Superficial vascularization.
Stage 3 – Healing stage
•Histiocytes and keratocytes convert into fibroblasts such that scar tissue is formed.
•Vascularization occurs at ulcer site; influx of fibroblasts and antibodies promote healing.
•Process of cicatrization occurs due to regeneration of collagen and formation of fibrous
tissue.
•Newly formed fibres are not laid down regularly ; a scar tissue is formed which reflects
light irregularly.
7.
Keratomycosis
1. It iscommon in tropical regions(rural and warm climates)
2. Molds tend to cause the majority of fungal ulcers in tropical and sub-tropical climates
while Candida, a dimorphic yeast, is the more common etiology of fungal ulcers in
temperate climates(4)
3. Fungi are opportunistic organism rarely affecting intact cornea but in compromised
and immunosuppressed state (ocular surface disease, topical steroid use or trauma
with vegetative matter)
4. In South India, the dominance of fungal keratitis, particularly
of Fusarium and Aspergillus, is prevalent more than a decade.(5)
5. In Northern India Aspergillus spp. were the most common causative agents
accounting for 25 (40.1%) of the isolates, followed by Fusarium sp. with ten (16.4%),
Curvularia sp. with five (8.2%), Candida albicans with five (8.2%) (6).
4.Keay LJ, Gower EW, Iovieno A, et al. : Clinical and microbiological characteristics of fungal keratitis in the United States, 2001–2007: a
multicenter study. Ophthalmology. 2011; 118:920–926.
5. 8.Bharathi M. J., Ramakrishnan R., Vasu S., Meenakshi R., Palaniappan R. Epidemiological characteristics and laboratory diagnosis of fung
al keratitis. A three-year study. Indian Journal of Ophthalmology. 2003;51(4):315–321.
6. Chander J, Sharma A. Prevalence of fungal corneal ulcers in northern India. Infection. 1994 May-Jun;22(3):207-9.
8.
(7)
7.Sharma, N., &Vajpayee, R. B. (2008). Corneal ulcer- diagnosis & management. Jaypee Brothers M
edical Publishers (P) Ltd.
9.
(8.)
8.Sharma, N., &Vajpayee, R. B. (2008). Corneal ulcer- diagnosis & management. Jaypee Brothers Medical Publishers (P) Ltd.
Gram stain showing Yeast cells Gram stain showing aspergillus
Aspergillus Fumigatus Fusarium species
Curvularia Alternaria
10.
Trauma – vegetable/ organic matter, plant matter
as leaves, paddy grains, injury with mud or sand,
injury from animal origin as cow dung, cow tail or
even with metal pieces.
Contact lens wearer
Indiscriminate use of topical steroids and topical
antibiotics; traditional eye medicines.
Surgeries- keratoplasty, cataract
surgery ,refractive surgery, penetrating keratoplasty
etc.
(9)
9.Sharma, N., & Vajpayee, R. B. (2008). Corneal ulcer- diagnosis & management. Jaypee Brothers Medical Publish
ers (P) Ltd.
11.
(10)
Fungal Keratitis afterVegetative Trauma Fungal keratitis after using traditional eye medicines
Fungal keratitis after Keratoplasty
10. Sharma, N., & Vajpayee, R. B. (2008). Corneal ulcer- diagnosis & management. Jaypee Broth
ers Medical Publishers (P) Ltd.
12.
General Symptoms -
A.The symptoms are less than what the size
would warrant.
B. Onset – insidious
C. Prolonged duration (5-10 days)
D. C/o Foreign body sensation for several days
with slow onset of increasing pain and DOV
E. Gradual onset of pain,
grittiness ,photophobia, blurred vision and
watery or mucopurulent
discharge,redness(circumcorneal congestion) Early fungal ulcer presenting with mild congestion
and few symptoms
13.
Signs :-
1. Yellowwhite stromal infiltrate
with indistinct fluffy
margins(Filamentous
Keratitis)
Candida Keratitis- Yellow
white densely suppurative
infiltrate.
14.
2. Yellowish white
infiltrateswith base filled
with soft , creamy and
raised exudates
Raised margins and creamy exudates
15.
3.Feathery branch
like extensionsor
margins or ring shape
infiltrate may develop.
Ring shape infiltrate
Corneal ulcer culture positive for
Fusarium ; typical broad feathery
infiltrate.
Early stage of fungal corneal ulcer in
which typical feathery
margins(PATHOGNOMIC) at 7 o’ clock
are progressing.
16.
The fungal ulcershave
characteristic findings,
which include elevated
areas, hyphate
(branching) ulcers,
irregular feathery
margins, a dry rough
texture and satellite
lesions.
Satellite lesions
Irregular feathery margins and dry texture Two central and two peripheral satellite
lesions
Main lesion with satellite lesion
17.
Hypopyon isthick,cheesy,immobile,non-sterile and
has convex surface
Endothelial plaque with perforation
An immune ring, endothelial plaque and a
posterior corneal abscess may be present rarely.
18.
Laboratory
Diagnosis
Specimen Collection –
Cornealscraping –
1. Using kimura spatula or a surgical blade
2. Corneal ulcer scrapings from the ulcer edge and the base form the mainstay of the
diagnosis of a case of fungal keratitis.
3. Corneal scraping not only provides diagnostic clues but also may be therapeutic
as it also aids in the initial debridement and debulking of the organisms
4. Material obtained is then inoculated in Sabouraud dextrose agar, Sheep Blood
Agar, Potato diffusion Agar , Brain Heart Infusion broth(11)
11.Prajna, L., Vijayakumar, Venkatesh Prajina, N., & Srinivasan, M. (2008). Aravind’s atlas of fungal corneal ulcers.
Jaypee Brothers Medical.
19.
Infected area gentlyscraped by using Kimura spatula
Corneal scraping collected by an Ophthalmologist using slit lamp microscope
Fungal culture (12)
Adefinitive diagnosis of fungal keratitis is made if
1. Corneal scrapings reveal fungal elements in smears.
2. Fungus grows in more than one medium in the absence of fungus in smears.
3. Fungus grows on a single medium in the presence of fungus in smears.
4. Confluent growth of fungus appears at the inoculated site on a single solid
medium.
(12)Salmon, J. F. (2024). Kanski’s clinical ophthalmology: A systematic approach (10th ed.). Churchill Livingstone
.
22.
1. Positive culturesshould be expected in 52
to 68 percent of cases.
2. Initial growth occurs within 72 hours in 83
percent of cultures and within 1 week in
97 percent of cultures.
3. Most in fact are visible with dissecting
microscope or naked eye within 36 hours.
But we should wait for at least a week before
declaring a culture negative for fungi(13)
Culture media showing growth of various fungi
13.Salmon, J. F. (2024). Kanski’s clinical ophthalmology: A syste
matic approach (10th ed.). Churchill Livingstone.
23.
• Corneal Biopsy(14)
1.Corneal biopsy is indicated in suspected fungal
keratitis in the absence of clinical improvement
after 3–4 days .
2. If no growth develops from scrapings after a
week.in Deep stromal lesions and in case of
endothelial plagues.
In operation theatre a 3-5mm circular trephine set to
outline the area to be biopsied to a depth of 0.2-0.3mm.
The edge of the specimen is lifted from forceps and
dissected.
The dissected part can be sent for histological analysis
and culture.
14. Salmon, J. F. (2024). Kanski’s clinical ophthalmology: A systematic approach (10th ed.). Churchill Livin
gstone.
Fungal elements stainsilver to black in Gomori Methamine stain
Blue white fluorescence in fungal hyphae in KOH calcofluor staining
27.
Newer Diagnostic Modalities
PCR(POLYMERASE CHAIN REACTION)-
Polymerase chain reaction (PCR) analysis of specimens is rapid and highly sensitive
(up to. 90%) and may be the current investigation of choice
This technique requires only 4 hours to obtain the results which is quicker than the 2
days to 2 weeks required by culture methods
ANTERIOR CHAMBER TAP has been advocated in resistant cases with
endothelial exudate, because organisms may penetrate the endothelium.
28.
CONFOCAL MICROSCOPY-
Confocal microscopyis an imaging technique that allows optical sectioning of almost
any material, with increased axial and lateral spatial resolution and better image
contrast, which may be useful for the identification of corneal pathogens in the early
stages of infection
29.
MANAGEMENT
The Mycotic UlcerTreatment Trial (15)
MUTT TRIAL I-
PURPOSE – Compared Natamycin 5% and Voriconazole 1% in patients with a
smear positive filamentous fungal ulcer and visual acuity of 20/40 to 20/400.
RESULT – Natamycin treated cases had significantly better 3 month BSCVA than
Voriconazole treated cases and better clinical and microbiological outcomes for
smear positive filamentous fungal keratitis.
15. Prajna NV, Krishnan T, Mascarenhas J, Rajaraman R et al; Mycotic Ulcer Treatment Trial Group. The
mycotic ulcer treatment trial: a randomized trial comparing natamycin vs voriconazole. JAMA
Ophthalmol. 2013 Apr;131(4):422-9. doi
: 10.1001/jamaophthalmol.2013.1497. PMID: 23710492; PMCID: PMC3769211.
30.
MUTT TRIAL 2(16)
OBJECTIVE – To determine whether there is clinical benefit with adjunctive use of
oral Voriconazole to topical antifungal eyedrops in the treatment of severe
filamentous fungal keratitis.
OUTCOME MEASURES-
Corneal perforation, need for therapeutic penetrating keratoplasty.
Culture negativity (6 days),BSCVA,complications associated with PO Voriconazole.
RESULT – The addition of oral Voriconazole to Topical antifungal eye drops in
the treatment of severe filamentous fungal corneal ulcers did not improve
clinical outcomes and increased the likelihood of adverse events.
16.Prajna NV, Krishnan T, Rajaraman R et al; Mycotic Ulcer Treatment Trial II Group. Effect of Oral Voriconazole
on Fungal Keratitis in the Mycotic Ulcer Treatment Trial II (MUTT II): A Randomized Clinical Trial. JAMA
Ophthalmol. 2016 Dec 1;134(12):1365-1372. doi
: 10.1001/jamaophthalmol.2016.4096. PMID: 27787540; PMCID: PMC6044431.
31.
MEDICAL THERAPY- (17)
1.Sincethe corneal epithelium serves as a barrier to the penetration of most tropical anti-fungal agents,
debridement of the corneal epithelium is an essential component of the medical management of fungal
keratitis
Initial drug of choice for fungal keratitis-
For Filamentous Fungi – (Drug of choice) 5% Natamycin Suspension
Given hourly during the day and two hourly during night time (taper slowly over 6-8 weeks)
Once the infiltrate started resolving, the frequency of topical natamycin is reduced to 2-hourly until
the completion of resolution .
The natamycin should be continued for 2 weeks after the resolution of infection in all cases.
17. Awad R, Ghaith AA, Awad K, Mamdouh Saad M, Elmassry
AA. Fungal Keratitis: Diagnosis, Management, and Recent Advances. Clin Ophthalmol. 2024 Jan 10;18:85-106. doi
: 10.2147/OPTH.S447138. PMID: 38223815; PMCID: PMC10788054.
32.
Candida - AmphotericinB( 0.15 percent) or Fluconazole( 0.3 percent )is the first drug of
choice or Nystatin eye ointment (3.5%)
2. Fluroquinolone(Broad Spectrum Antibiotic) may be given to prevent secondary bacterial
infection.
3. Cycloplegics such as homatropine eye drops may be given three times a day to relieve the
component of iridocyclitis
4. Antiglaucoma medications if IOP increases.
Voriconazole is an azole drug that is derived from fluconazole. It is proven to be a broad-
spectrum antifungal for both filamentous and yeast fungi.
The minimal inhibitory concentration of voriconazole is 0.5 μg/mL, which is less than that of
other imidazole drugs. It is considered a good alternative to natamycin in resistant cases.
33.
Candida - AmphotericinB( 0.15 percent) or Fluconazole( 0.3 percent )is the first
drug of choice or Nystatin eye ointment (3.5%)
2. Fluroquinolone(Broad Spectrum Antibiotic) may be given to prevent secondary
bacterial infection.
3. Cycloplegics such as homatropine eye drops may be given three times a day to
relieve the component of iridocyclitis
4. Antiglaucoma medications if IOP increases.
Reference -Sharma N, Sahay P, Maharana PK, et al. Management algorithm for fungal keratitis: the TST (top
ical, systemic, and targeted therapy) protocol.
Cornea. 2019;38(2):141–145.
SYSTEMICANTIFUNGAL
AGENTS-
In cases ofvery large ulcers, severe deep keratitis, scleritis and endophthalmitis.
The drugs, which have been used systemically, include
Ketoconazole (oral),miconazole (intravenous), itraconazole (orally 200 mg/day) and
fluconazole (orally 200 mg/day).Oral voriconazole 200 mg bd
Oral ketoconazole 600 mg per day. It is mandatory to assess liver function tests
every 2 weeks after starting ketoconazole. Systemic therapy is given for a period of 6
to 8 weeks
Topical corticosteroid in the treatment of fungal keratitis should not be used.
Reference-Awad R, Ghaith AA, Awad K, Mamdouh Saad M, Elmassry
AA. Fungal Keratitis: Diagnosis, Management, and Recent Advances. Clin Ophthalmol
. 2024 Jan 10;18:85-106. doi: 10.2147/OPTH.S447138. PMID: 38223815; PMCID: PMC10788054.
36.
Intracameral amphotericin Bmay be a useful modality in the treatment of severe
keratomycosis not responding to topical natamycin
For non healing fungal corneal ulcers is the use of intracameral Amphotericin B
injection in 5-7.5 μg dosage, given in the vicinity of the stromal site of fungal
growth.
37.
Resolution of fungalkeratitis in Intracameral Amphotericin B
Resolution of fungal keratitis in Intrastromal Amphotericin B
38.
SURGICALTHERAPY
Daily debridement witha spatula or blade is the simplest form of surgical
intervention and is usually performed at the slit lamp under topical anesthesia.
Debridement is performed every 24 to 48 hours and works by debulking organisms
and necrotic material and by enhancing the penetration of the topical antifungal
Biopsy may be used not only for the diagnosis but also as a therapeutic intervention
39.
When progression ofthe keratitis is noted, Penetrating keratoplasty should be
performed.
Therapeutic keratoplasty should be performed in cases of impending perforations,
frank perforations > 2 mm or if there is no response to therapy.
Non resolving fungal keratitis on maximum fungal medications on which therapeutic keratoplasty was done
40.
Sequelae and Complications:-
•Corneal ulcers involving the superficial lamellae generally heal by varying degrees
of scarring depending on the severity of inflammation. However, if the infection is
severe, there may be thinning, formation of a descemetocele, perforation.
•Corneal Opacification- Depending on the depth of the corneal ulceration, diffe rent
types of corneal opacities may occur that is, nebular, macular (> 50% involvement)
or leukomatous (> 75% involvement)
Healing corneal ulcer
with end stage
leukomatous corneal
opacity
41.
•Some corneal ulcersextend rapidly in depth so that the entire thickness of the cornea
except Descemet’s membrane is spared. The Descemet’s membrane like any other
elastic membrane offers resistance to the inflammatory process, but is unable to
withstand the intraocular pressure and therefore herniates through the corneal ulcer as
a transparent membrane called as descemetocele or a keratocele.
•Corneal Perforation-Pseudo Cornea & Corneoiridic Scar