This document discusses fungal keratitis, including its pathogenesis, classification, predisposing factors, clinical features, investigations, treatment, and recent advances. Some key points:
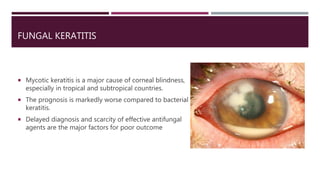
- Fungal keratitis is a major cause of corneal blindness in tropical areas and has a worse prognosis than bacterial keratitis due to delayed diagnosis and lack of effective antifungal agents.
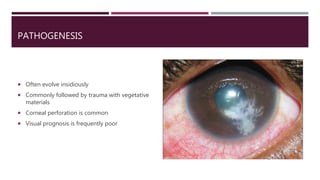
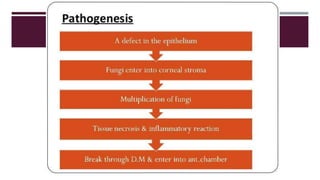
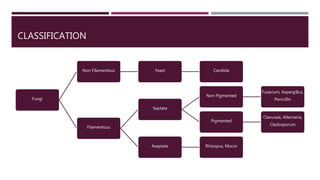
- It is commonly caused by trauma with plant materials and can lead to corneal perforation. Classification includes yeasts like Candida and filamentous fungi.
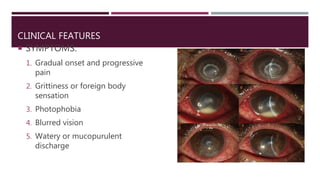
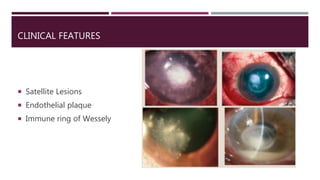
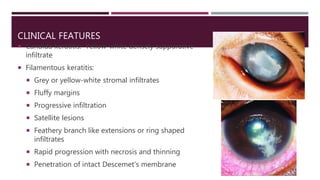
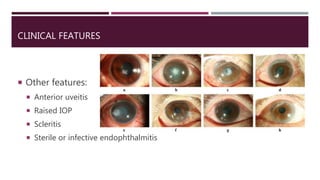
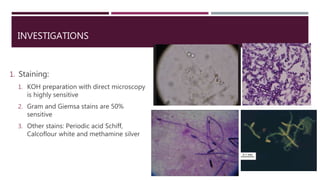
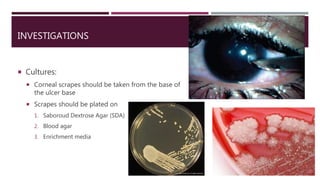
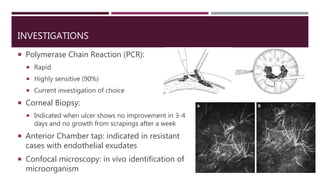
- Clinical features include pain, discharge, ulcers with feathery edges, and satellite lesions. Diagnosis involves staining, cultures, and PCR of corneal scrapes.
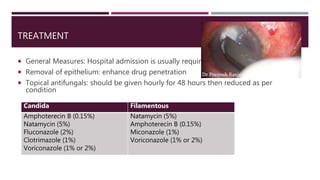
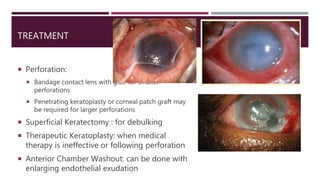
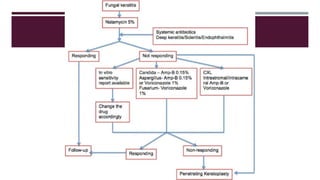
- Treatment