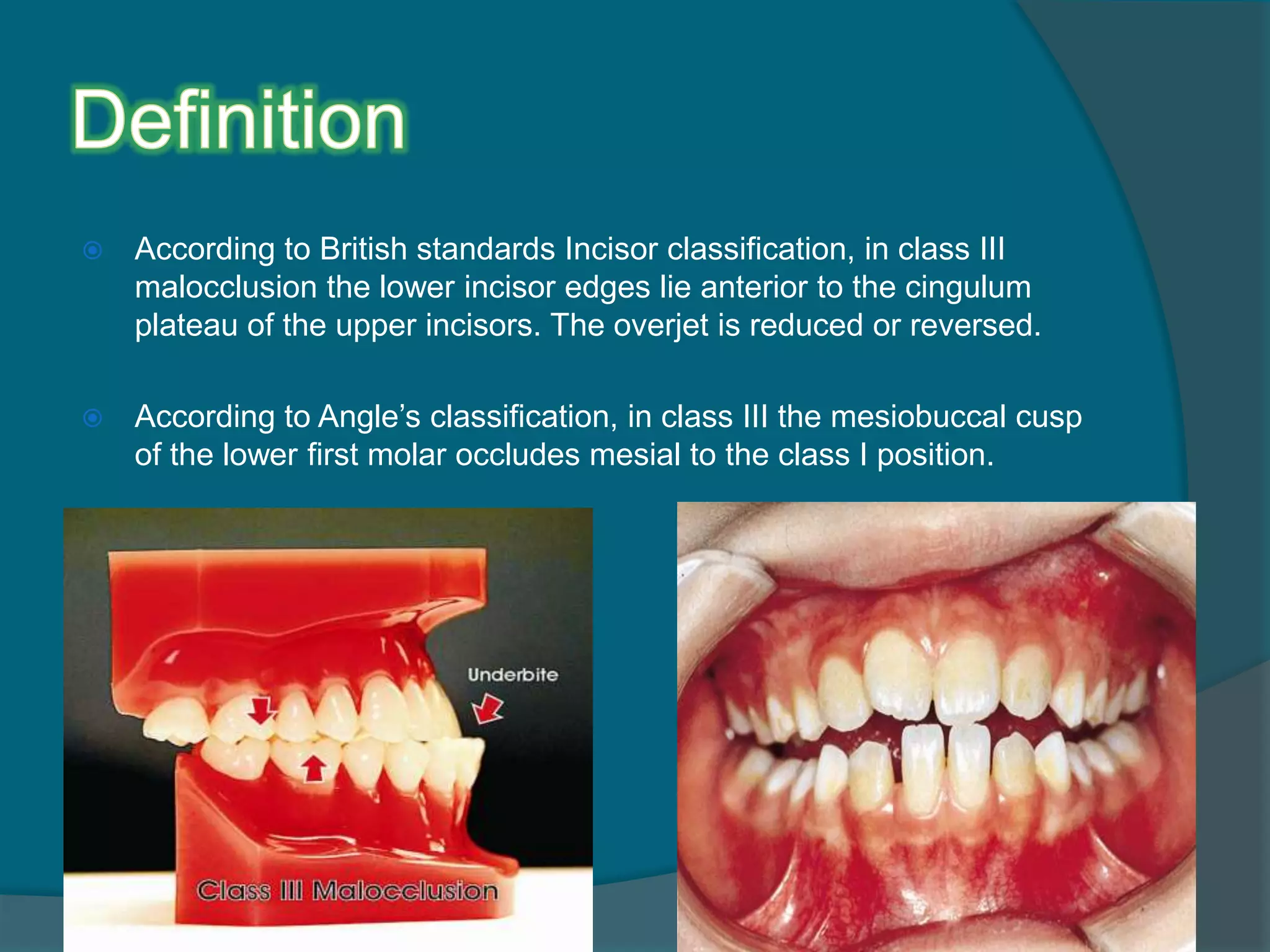
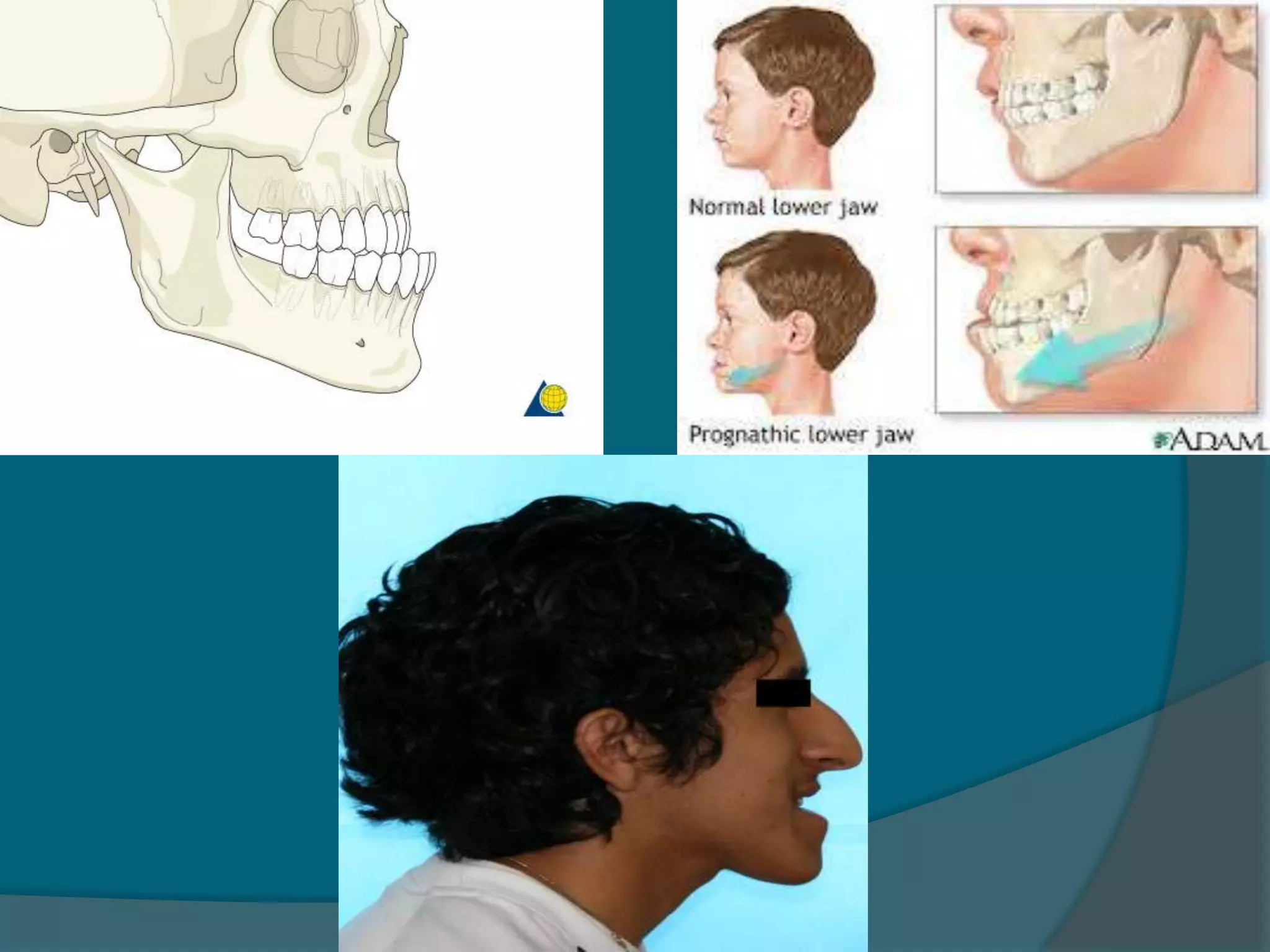
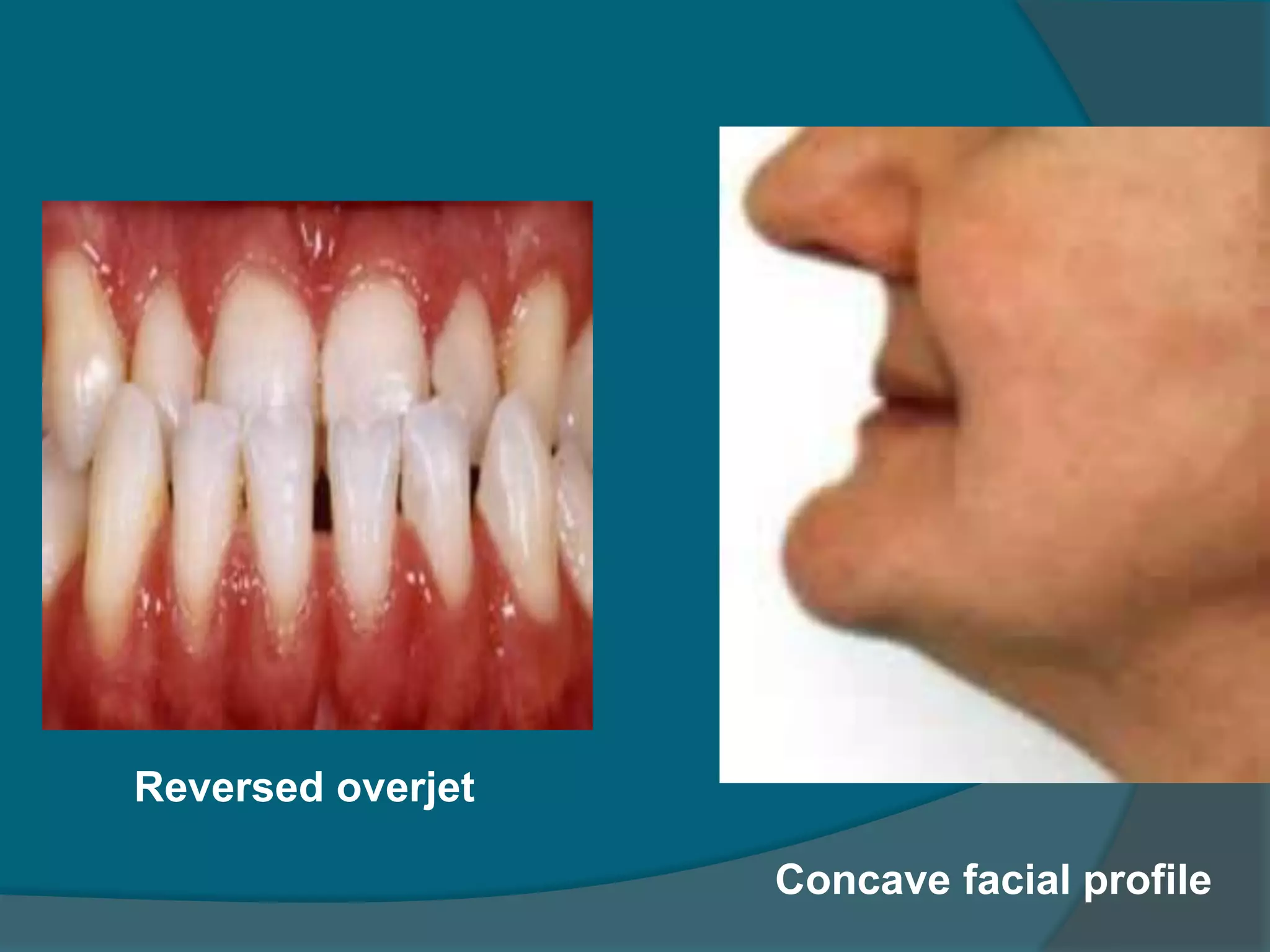
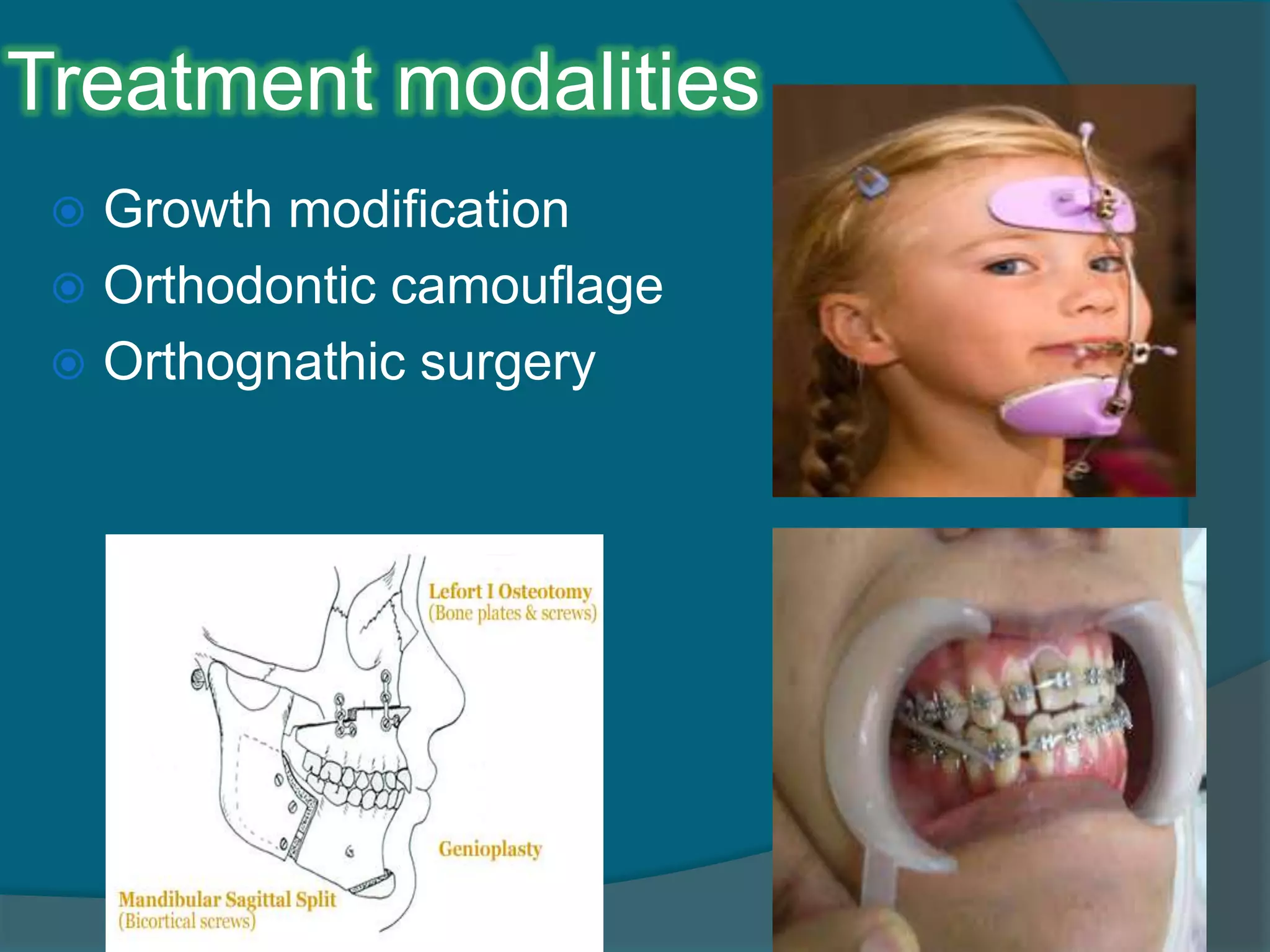



1. Class III malocclusion is characterized by the lower incisors positioned anterior to the upper incisors with a reduced or negative overjet. 2. The main causes are skeletal patterns like mandibular prognathism, maxillary retrognathism, or a combination of both. 3. Treatment depends on the severity and can include growth modification with functional appliances, orthodontic camouflage, or orthognathic surgery.

















































































