Downloaded 54 times


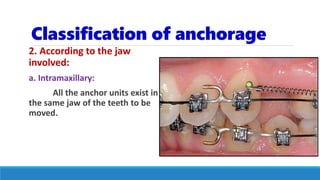
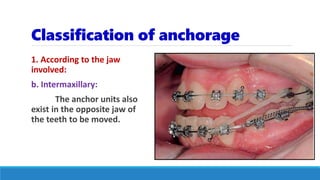
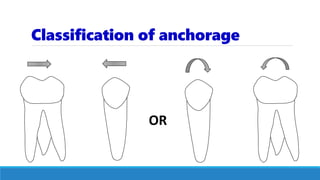
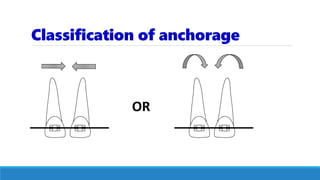
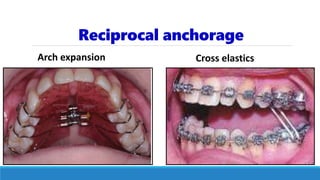



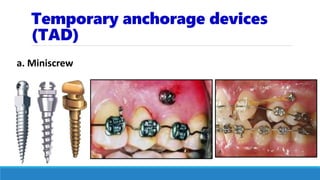
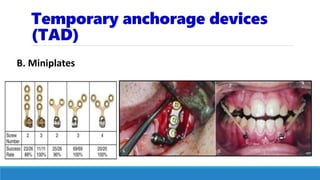

This document discusses anchorage in orthodontics. It defines anchorage as resistance to unwanted tooth movement. Sources of anchorage include intraoral teeth and bone, as well as extraoral structures like the occipital and cervical bones. The value of a tooth as an anchorage unit depends on factors like the number of roots, root size and length, periodontal support, root form, and tooth inclination. Anchorage can be classified based on site, jaw involved, number of units, and manner of force application. Reinforcing anchorage involves adding teeth to the anchorage unit, moving teeth gradually, using light forces, and employing devices like lingual arches, TADs, and extraoral appliances. Anch










































![lecture_05_and_06-Anchorage_in_orthodontics[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/lecture05and06-anchorageinorthodontics1-240224004209-047377b5-thumbnail.jpg?width=640&height=640&fit=bounds)




































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)







