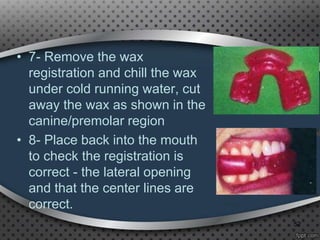
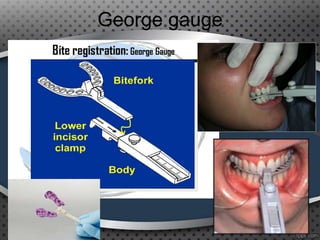
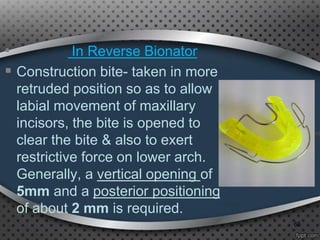
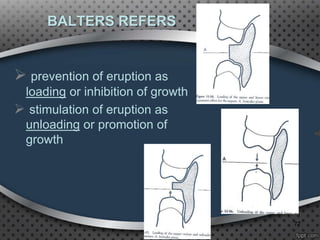
The document is a comprehensive overview of the bionator, a functional appliance used in orthodontics to aid in the growth of the mandible and correct various dental issues such as overbite and overcrowding. It details the history, types, construction, clinical management, and modifications of bionators, emphasizing their role in stimulating muscle activity and maximizing oral space for proper dental alignment. Additionally, it outlines specific design features and recommendations for effective use and maintenance of bionators in dental treatment.