Downloaded 70 times


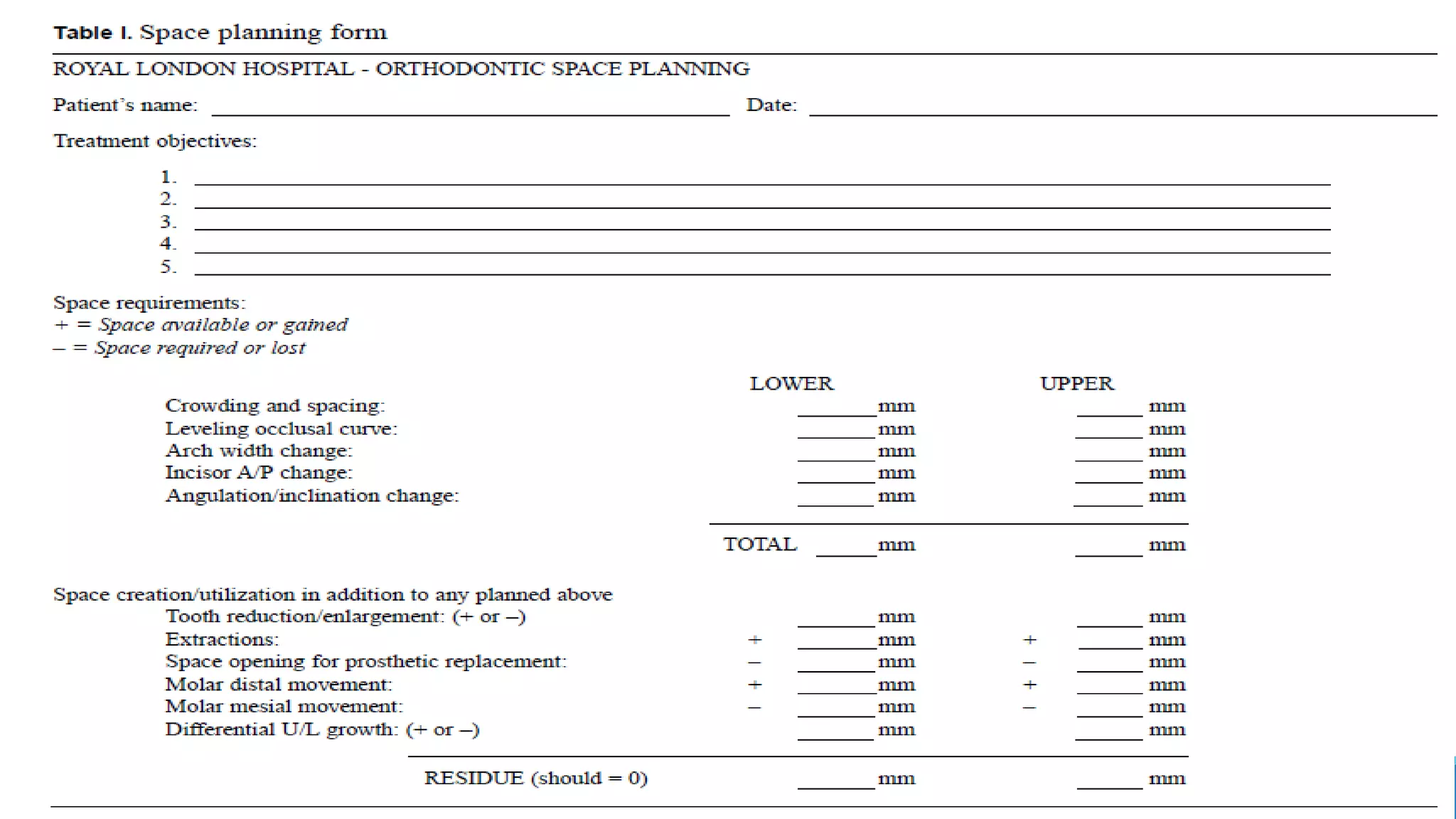
























The document discusses the Royal London Space Planning process for orthodontic treatment planning. The process occurs in two stages: 1) assessing the initial space required to achieve treatment objectives, and 2) integrating space analysis with consideration of how other treatment procedures may affect space. These procedures include tooth enlargement or reduction, extractions, replacing absent teeth, and molar movement. The analysis records any additional space created or used. The outcome is determining if treatment objectives can be attained with the planned mechanics.























































































