Download to read offline




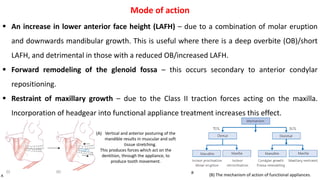
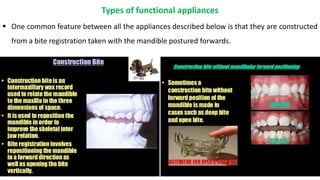


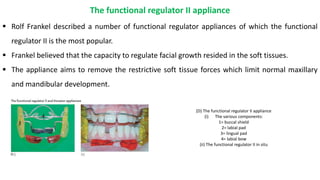
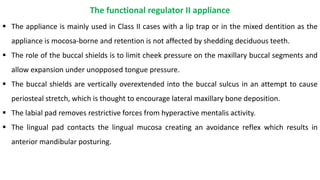

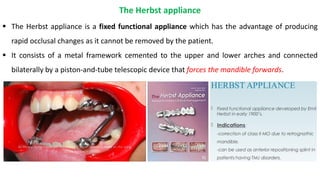

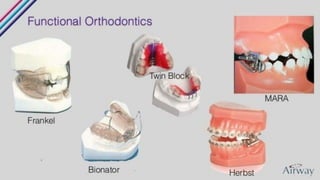

Functional appliances can be used to treat Class II malocclusions by altering mandibular posture. They work by stretching soft tissues and generating corrective forces through intermaxillary traction. This causes dentoalveolar changes like incisor angulation as well as skeletal effects like increased mandibular length. Common functional appliances include the twin block, functional regulator II, and bionator, which guide mandibular positioning through occlusal coverage or soft tissue contacts. The Herbst appliance is fixed to achieve rapid correction through an immovable telescopic connection between upper and lower components.






















































































