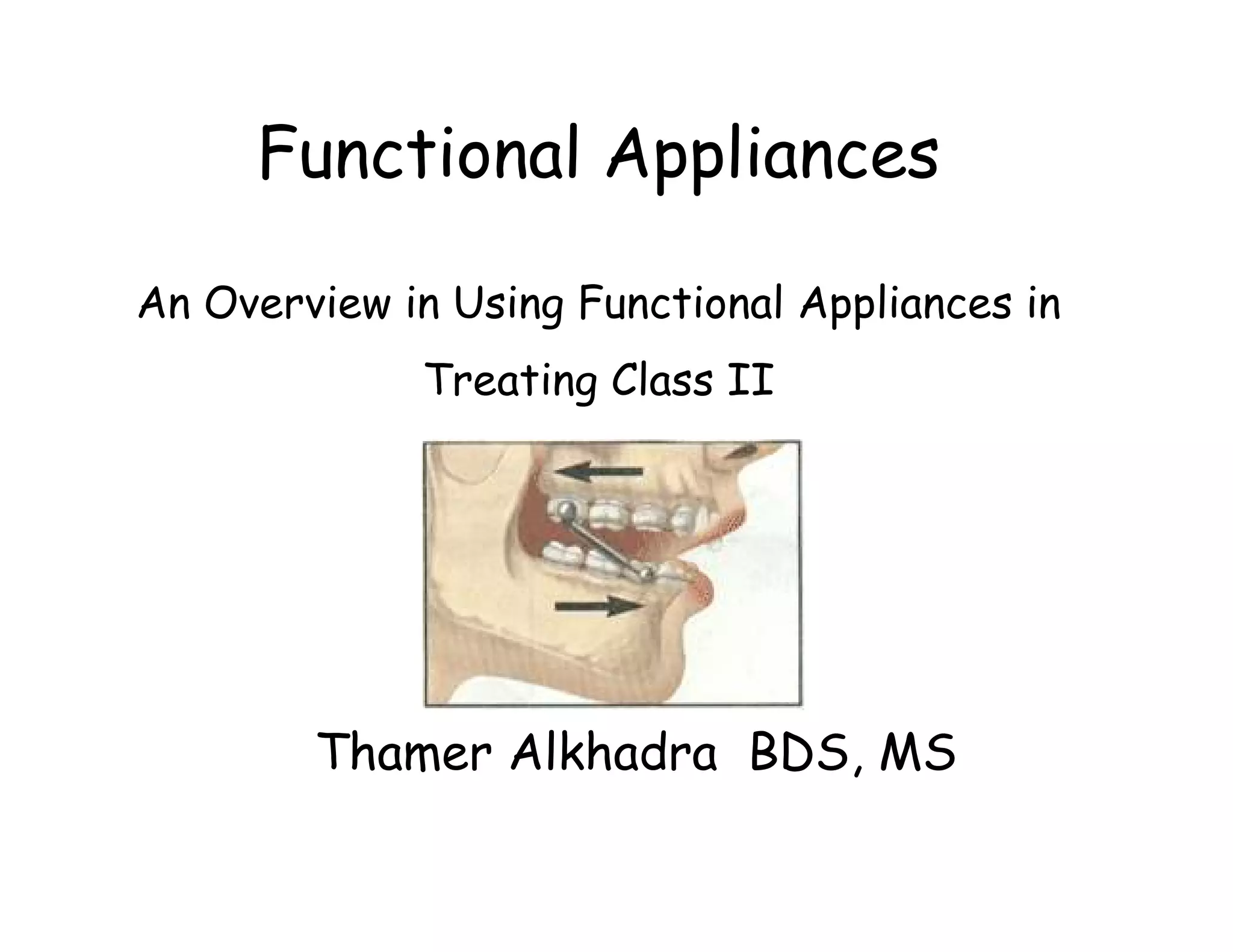
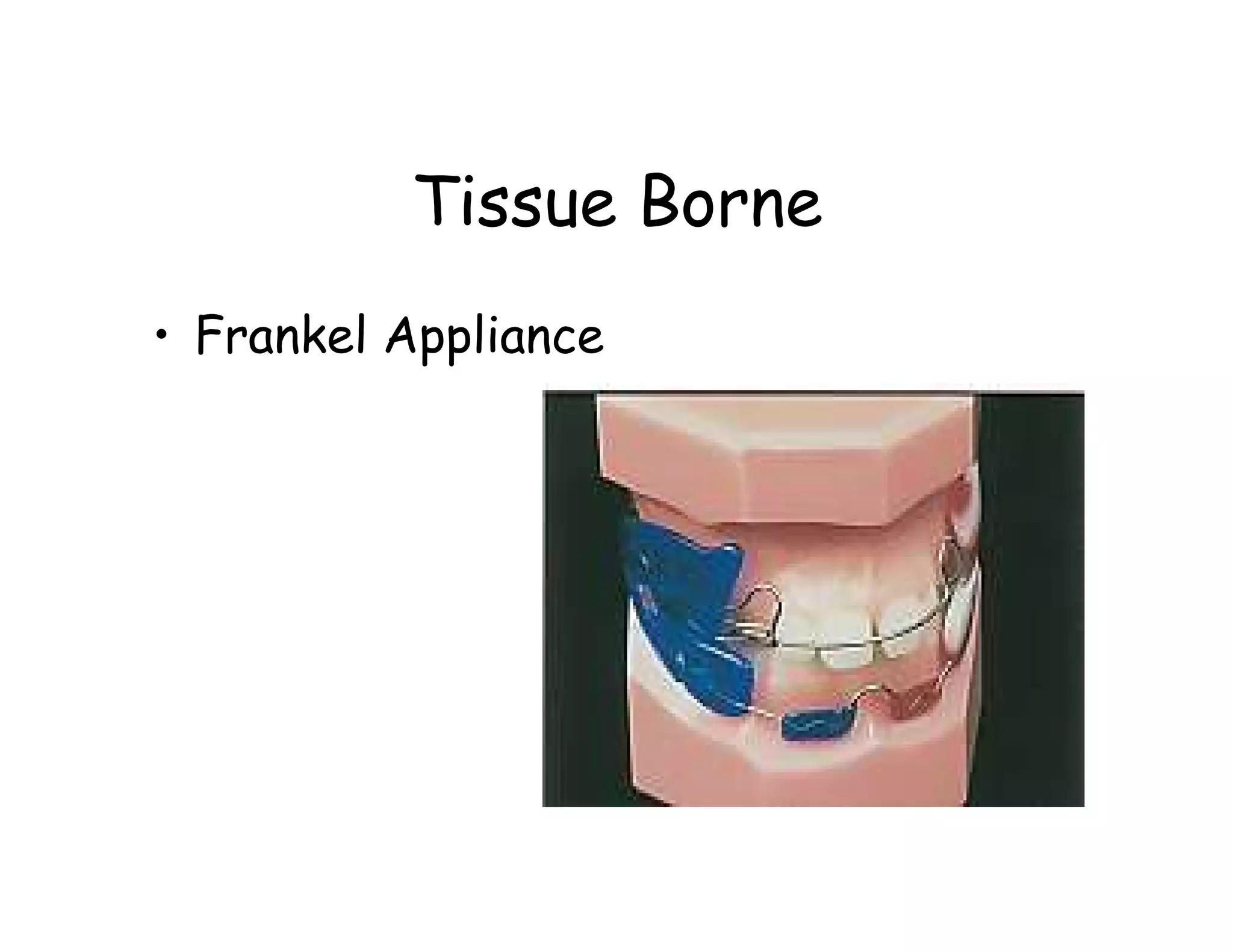
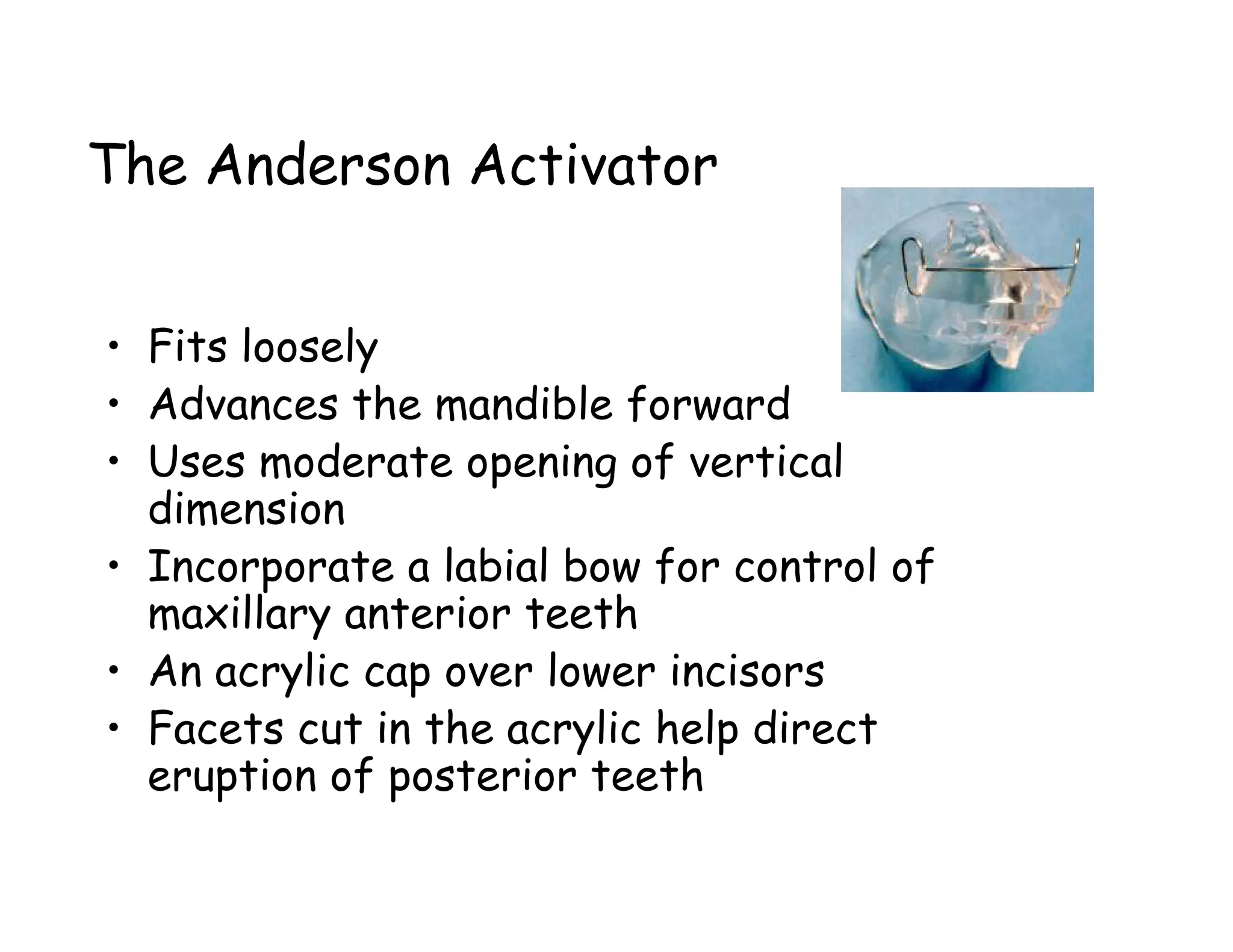
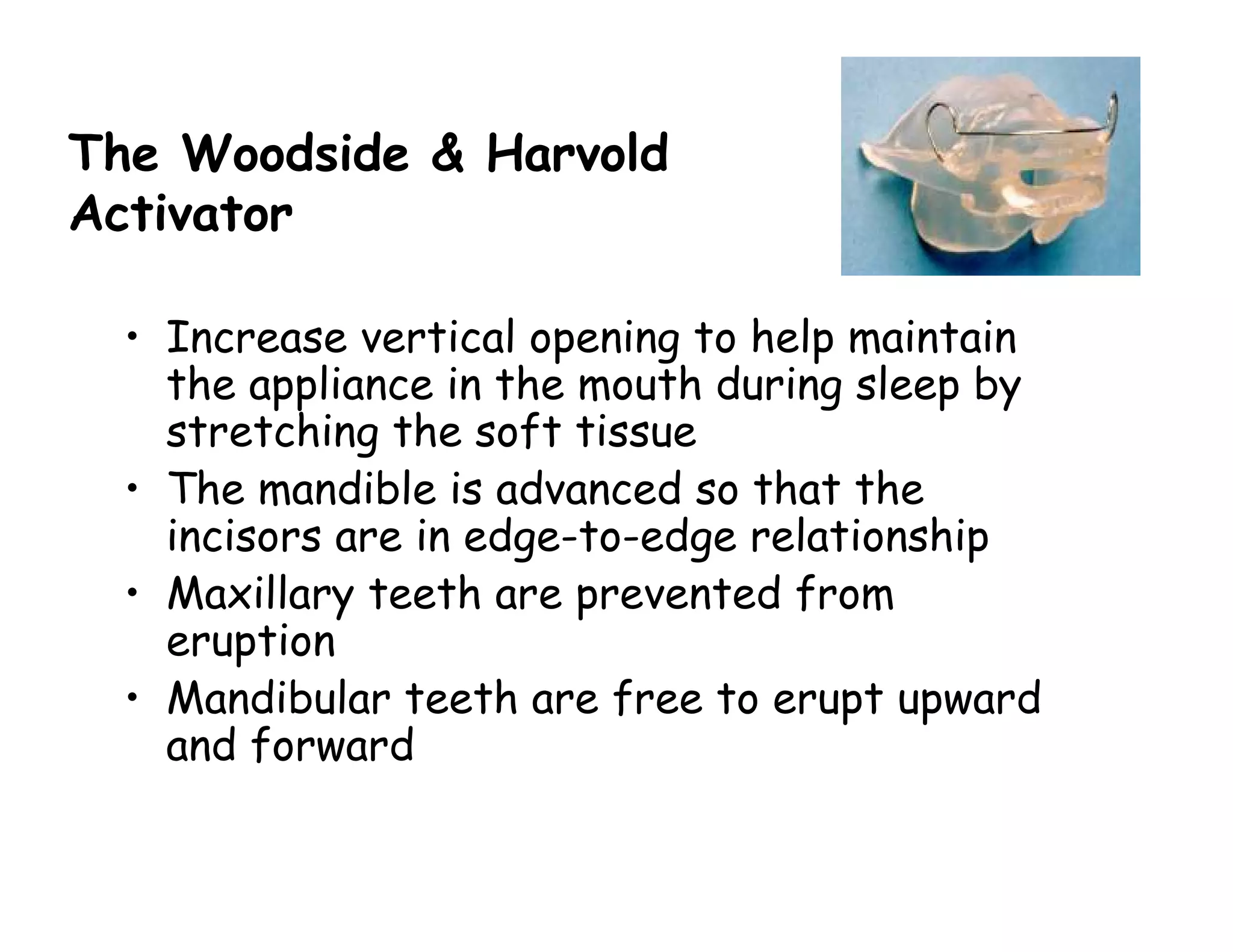
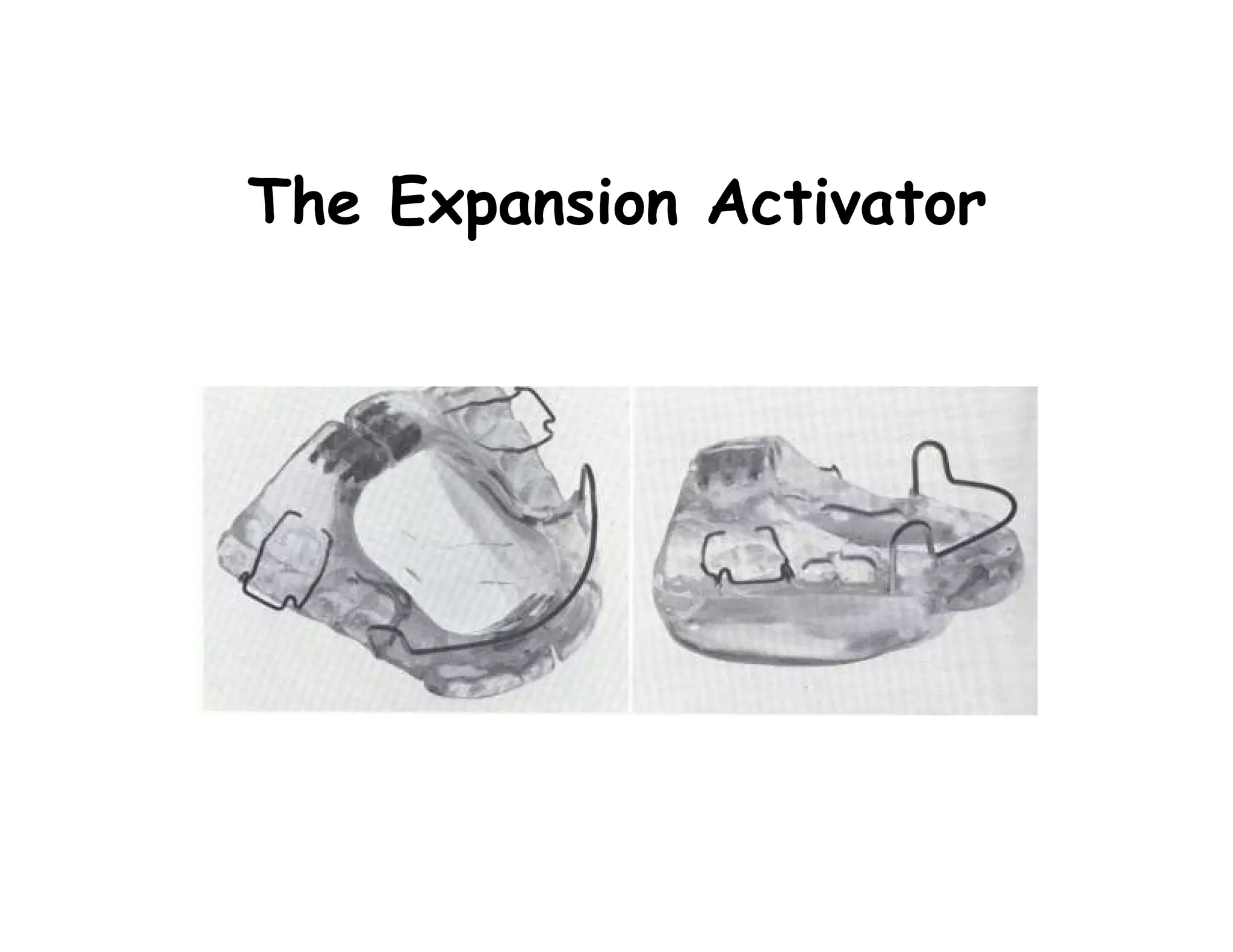
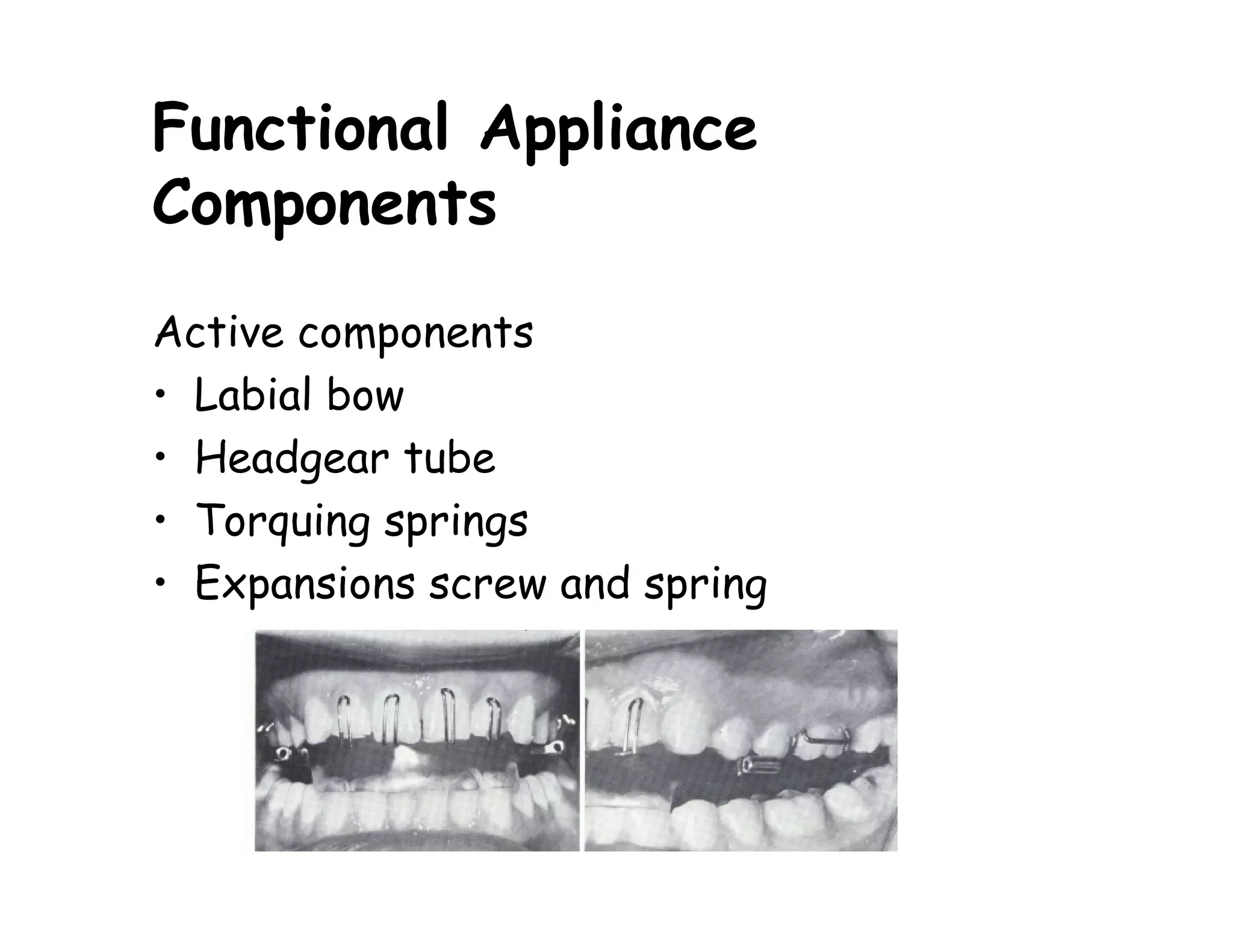
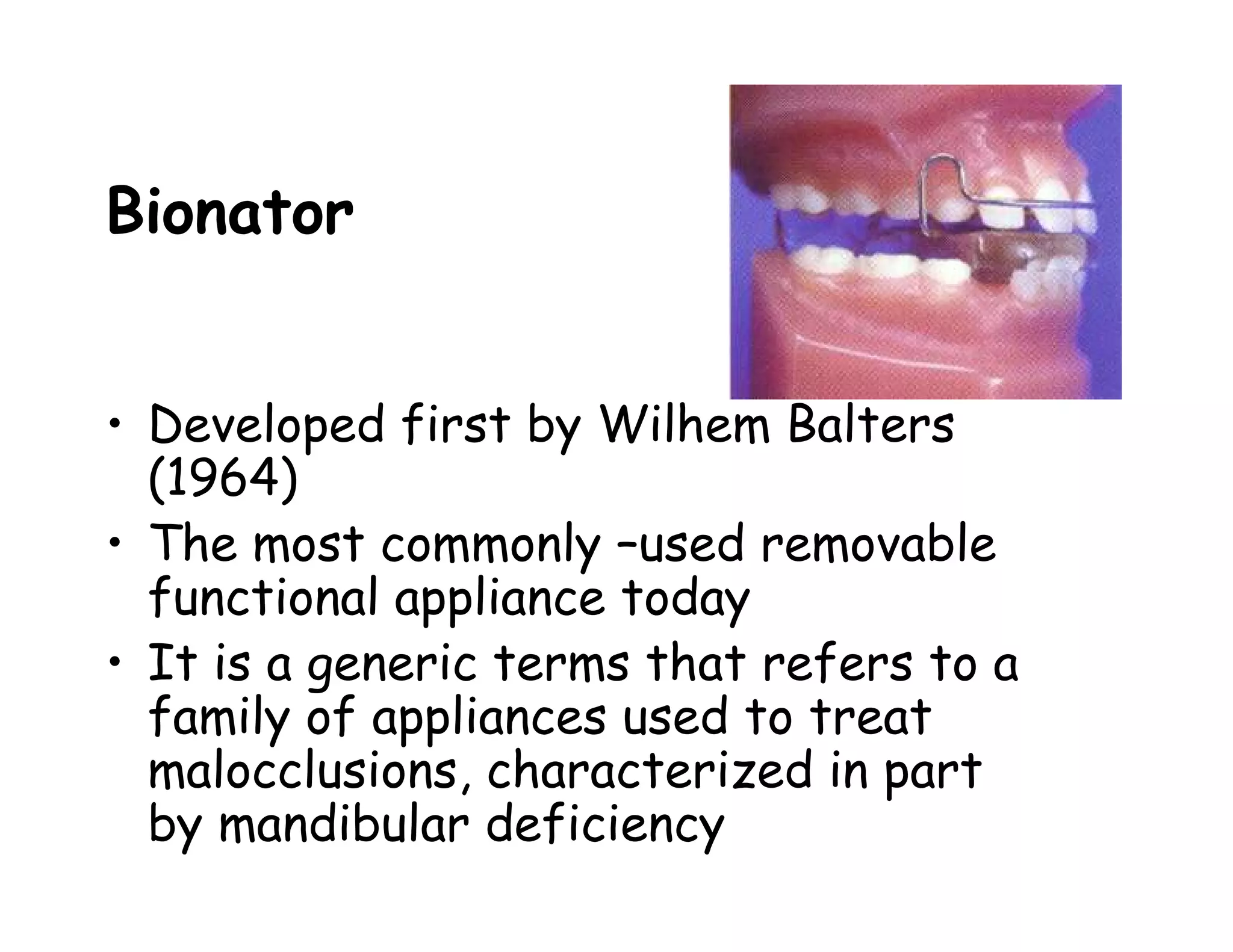
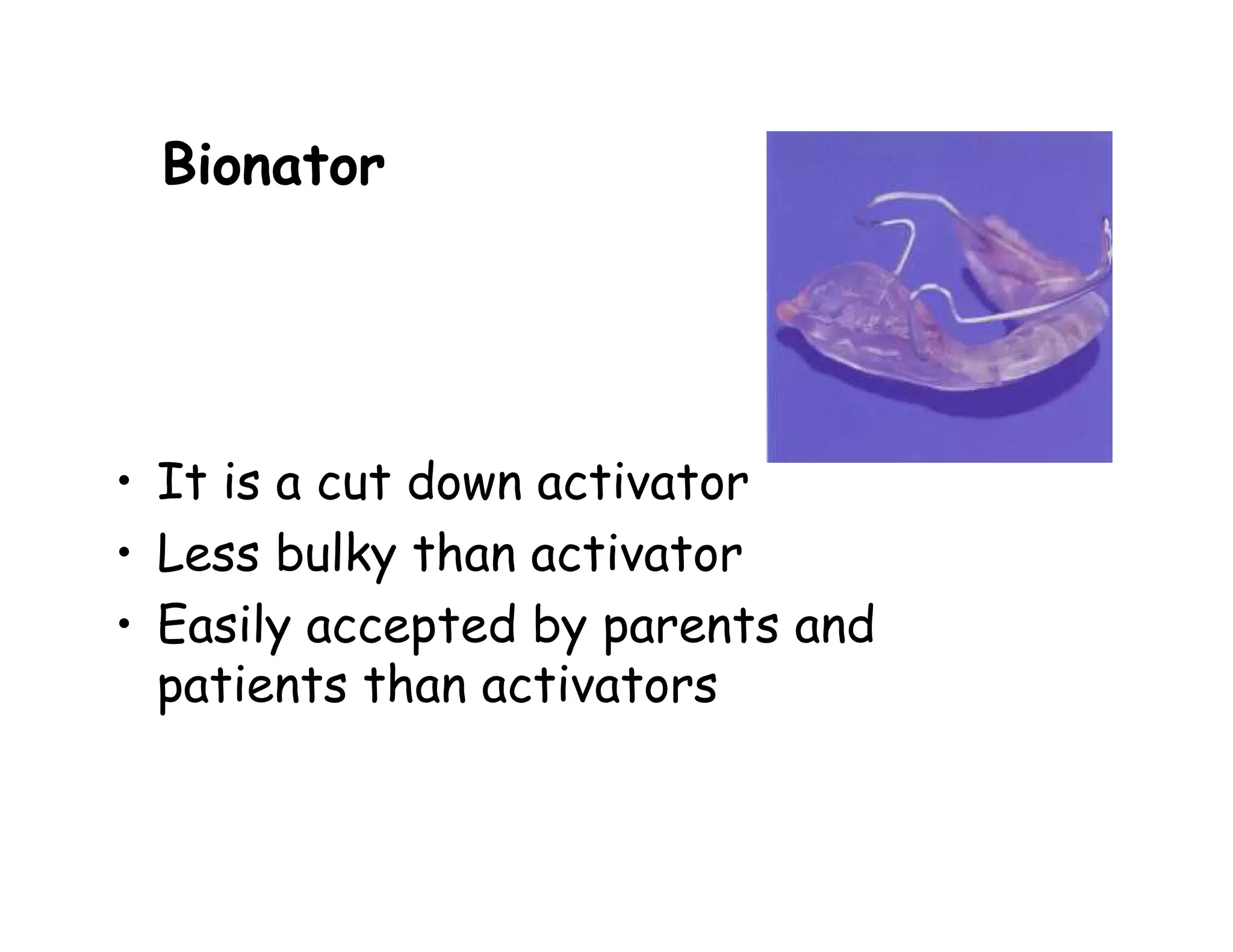
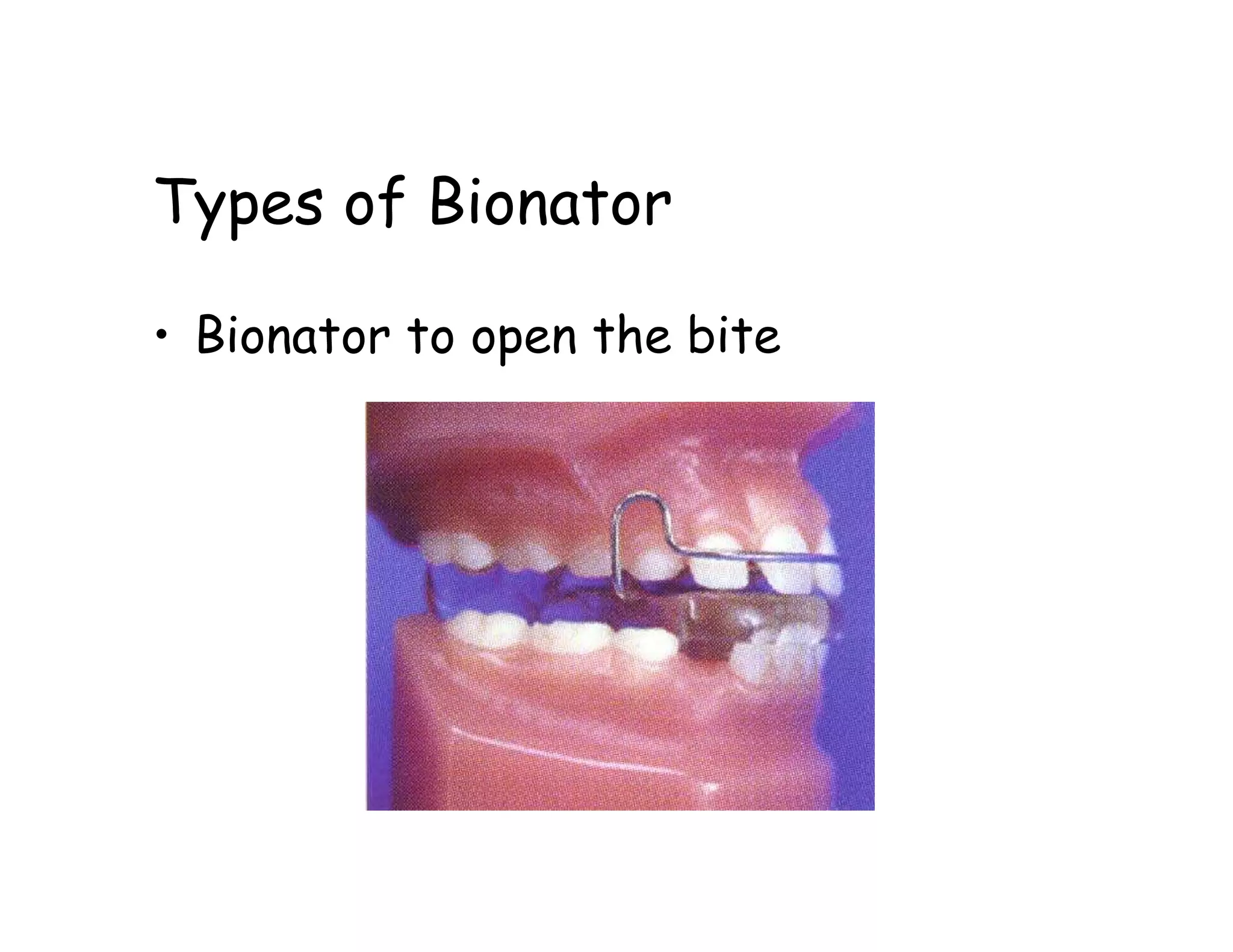
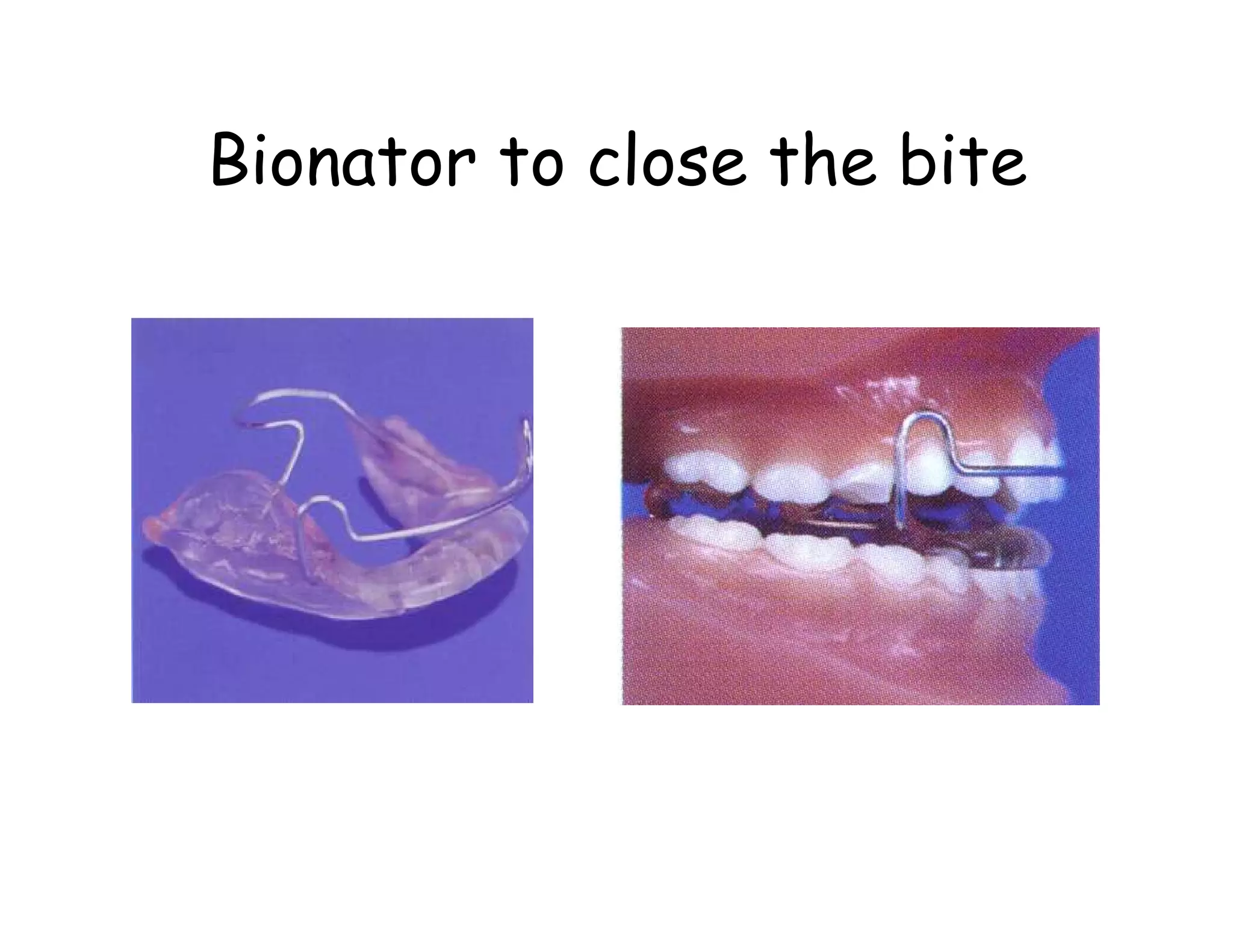
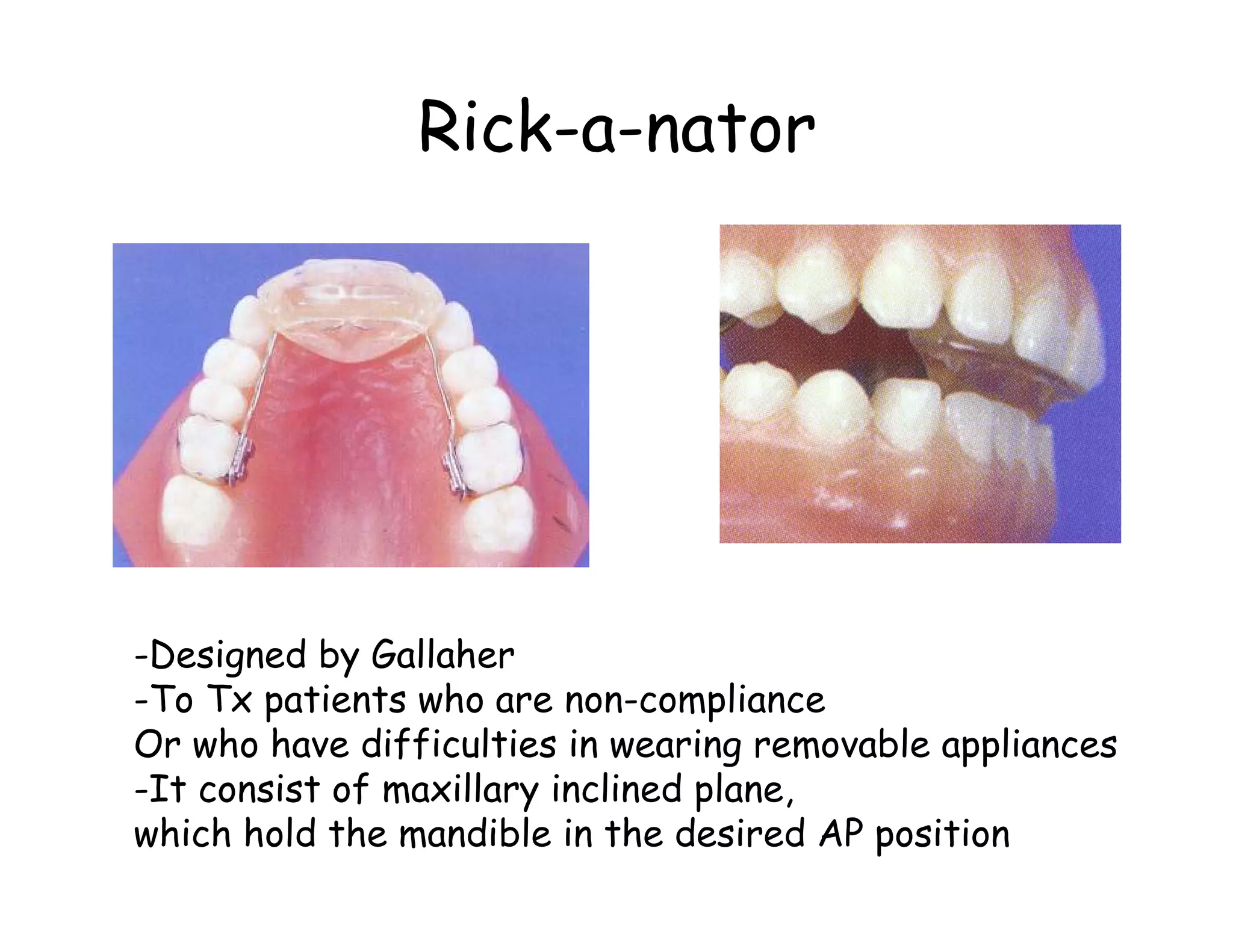
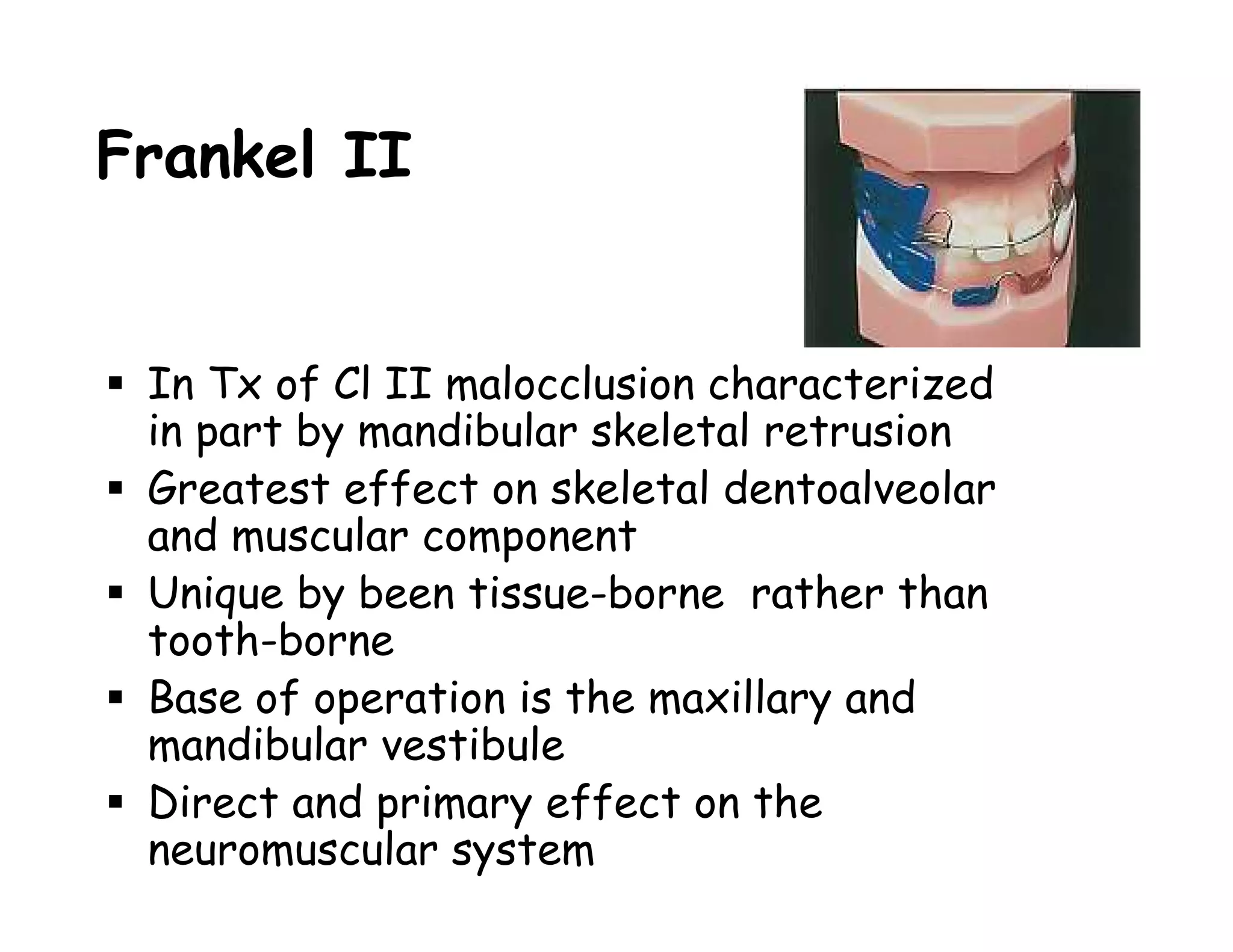
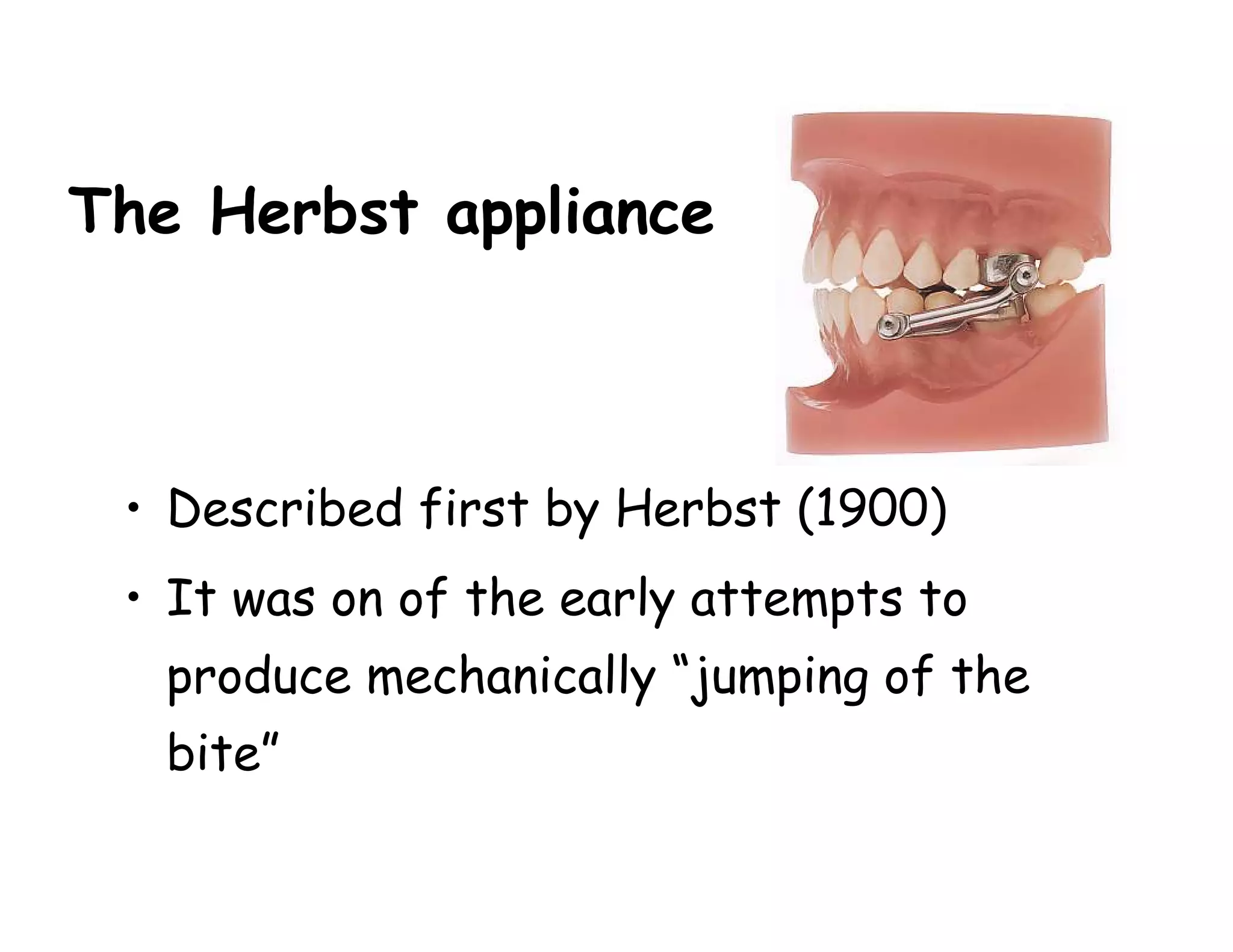
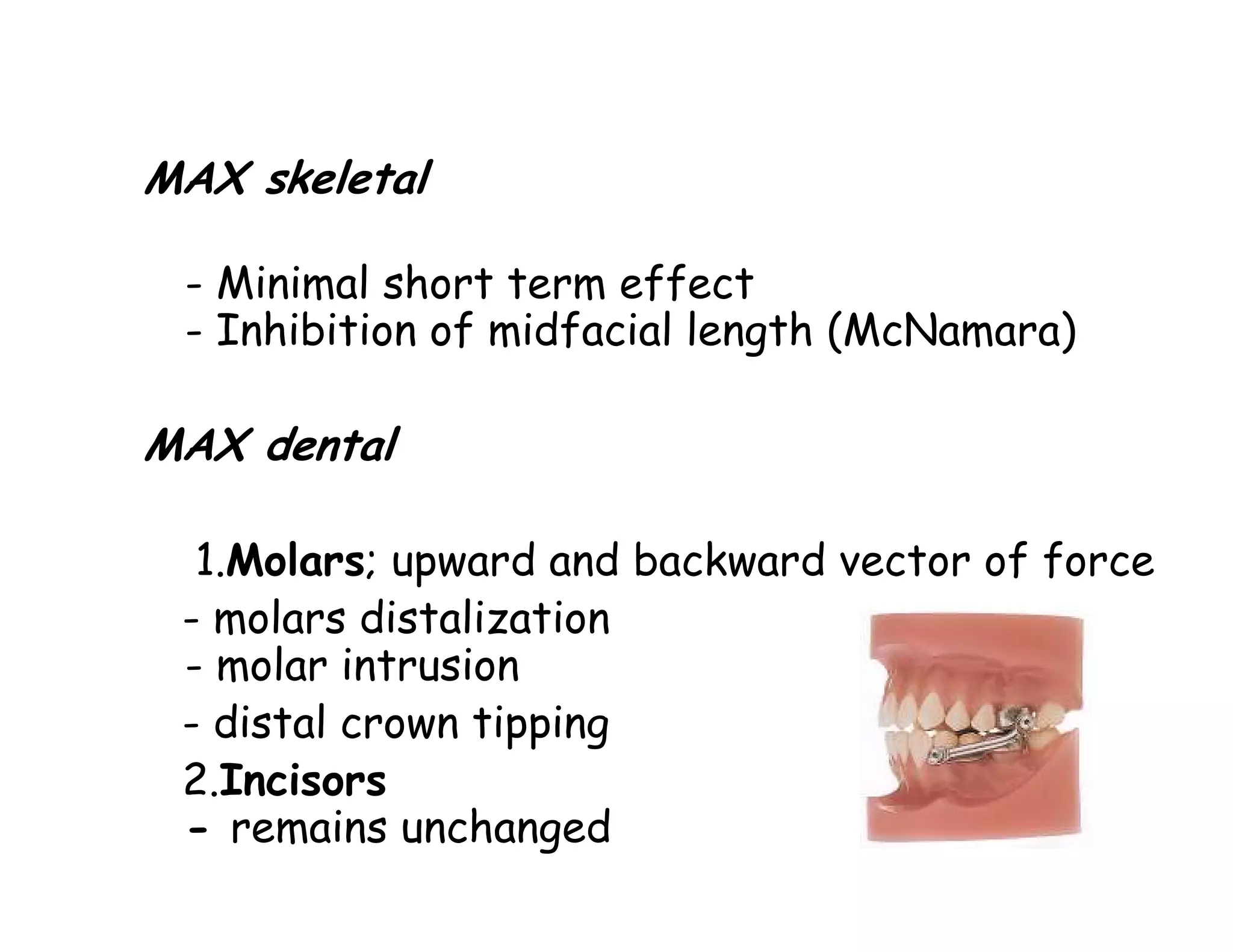
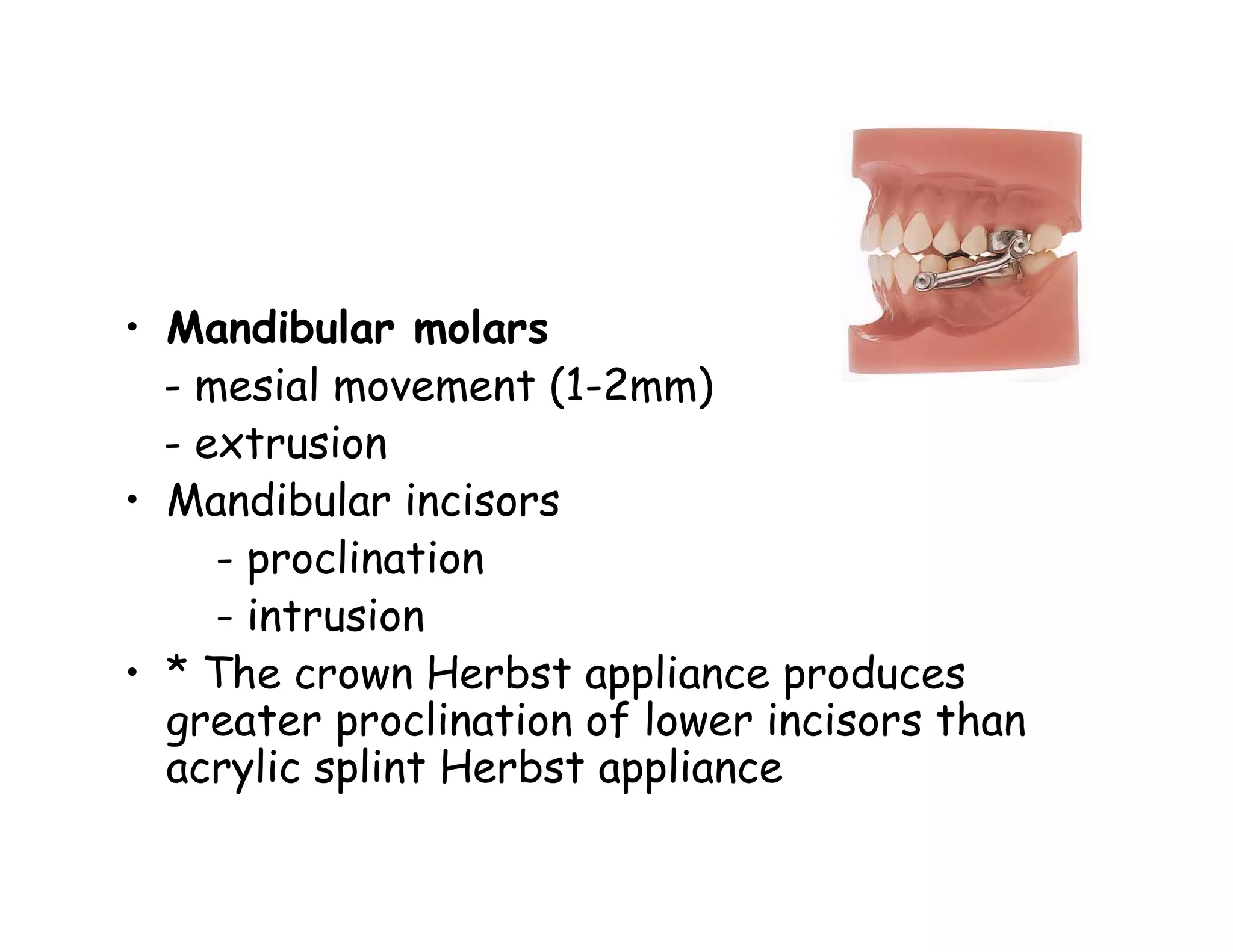
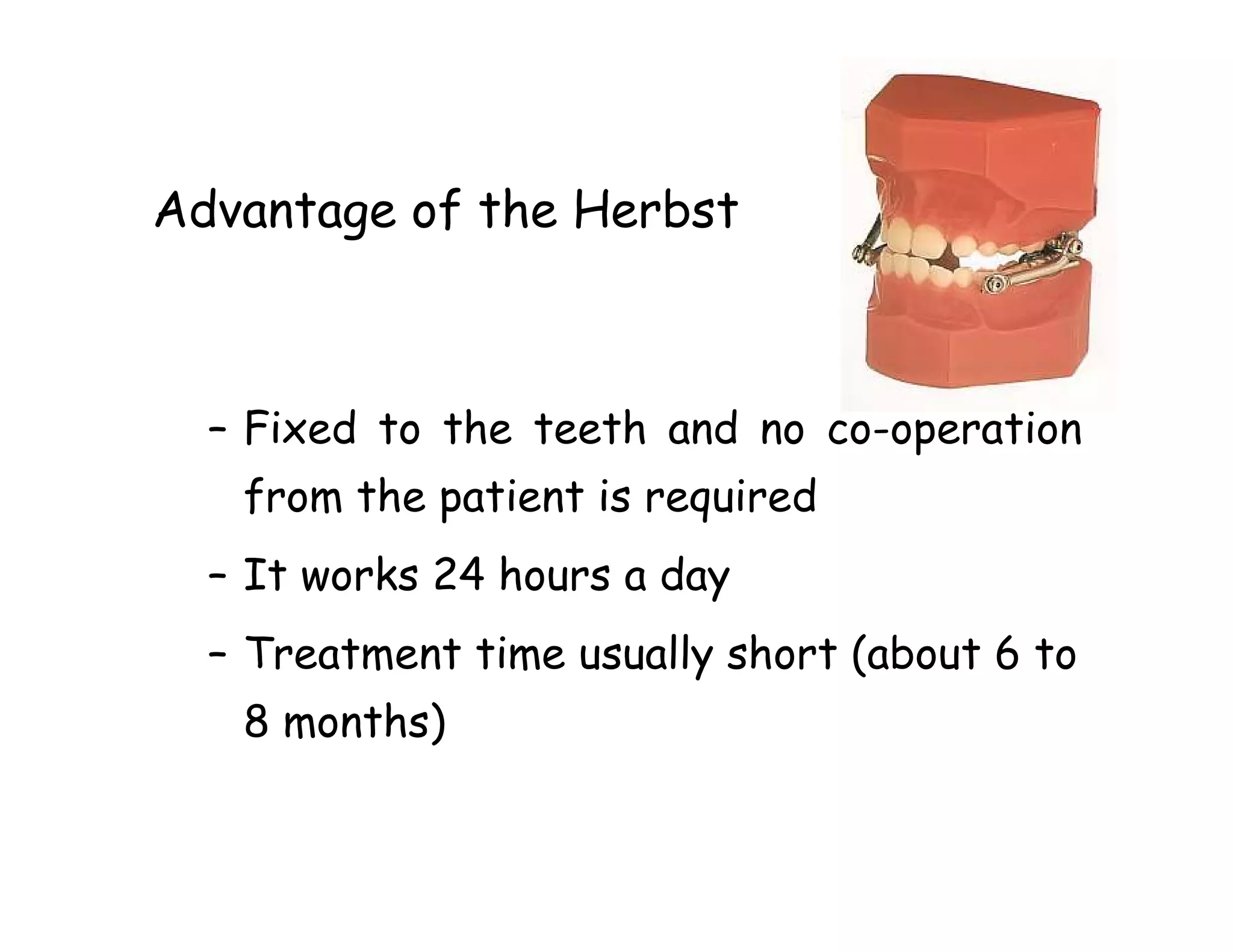
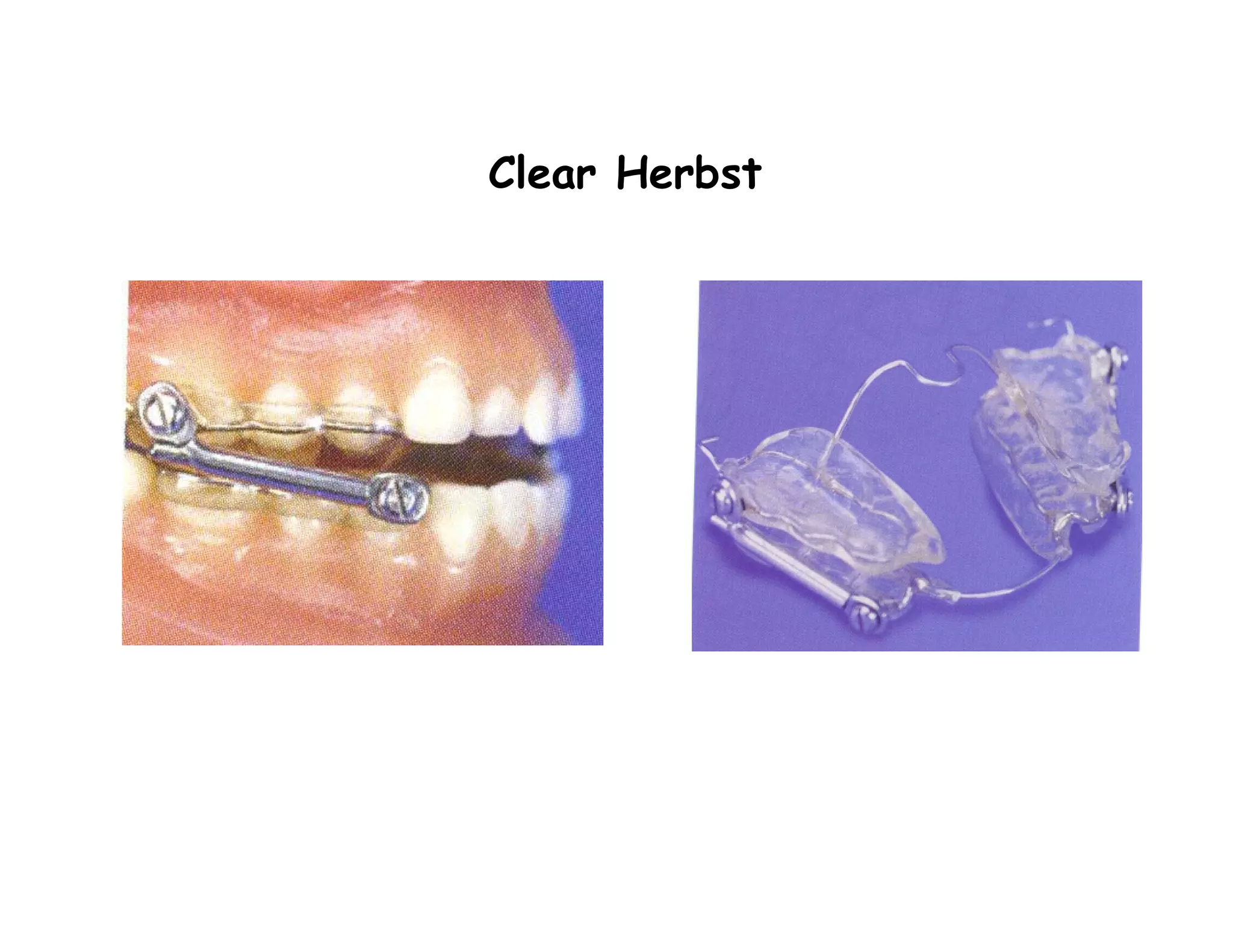
Functional appliances can be used to treat Class II malocclusions by altering mandibular growth and position. There are several types of functional appliances including removable appliances like activators and bionators, and fixed appliances like the Herbst appliance. Functional appliances work by transmitting natural forces to guide mandibular growth and positioning rather than directly acting on teeth. Common effects include proclination of lower incisors, retraction of upper incisors, and distalization of upper molars. Literature reviews have found functional appliances to be effective options for treating Class II malocclusions with both dentoalveolar and skeletal effects.