Downloaded 174 times

















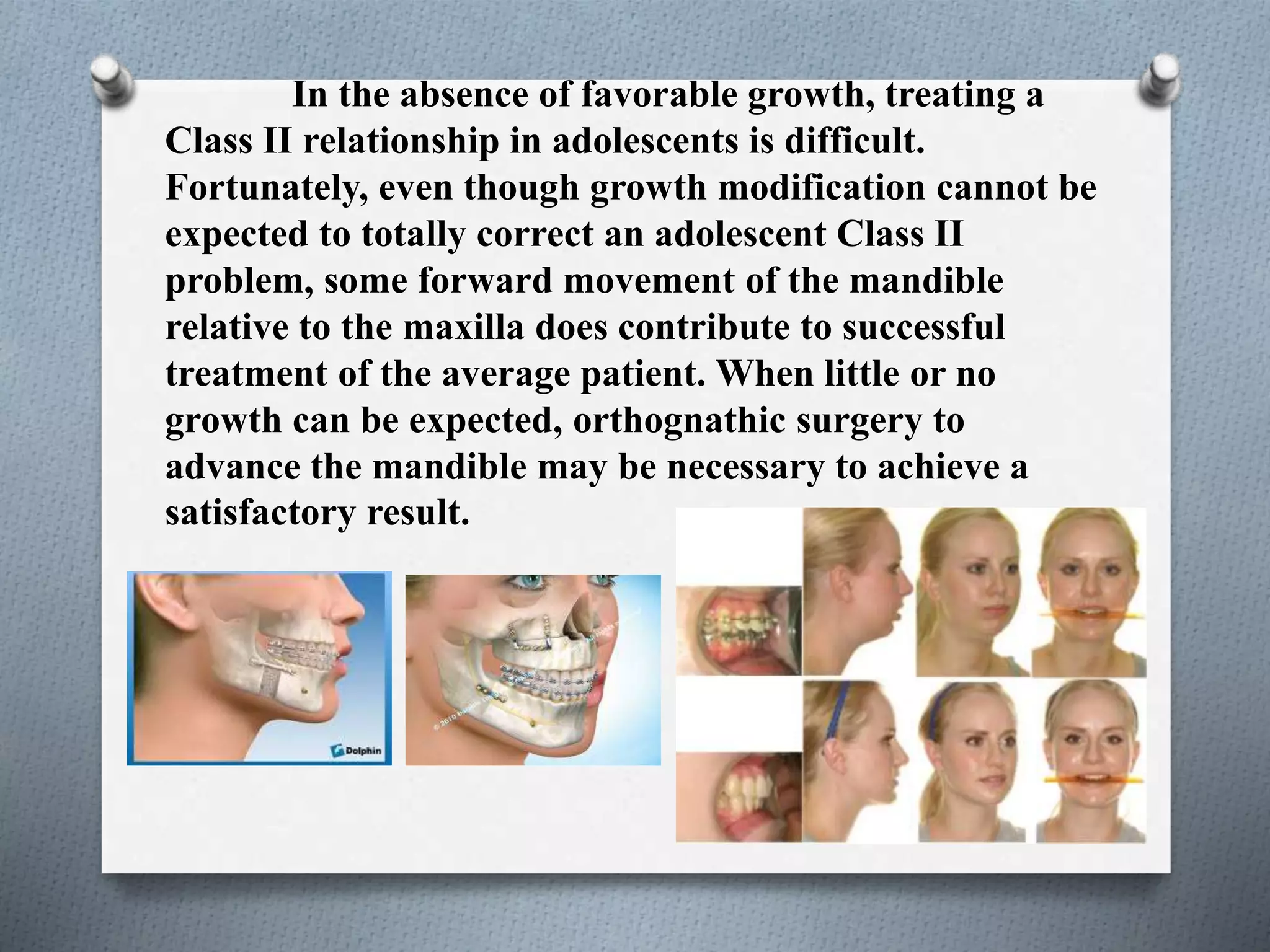


There are three main patterns of tooth movement that can be used to correct a Class II malocclusion: 1) nonextraction treatment with Class II elastics, 2) retraction of the upper incisors into a premolar extraction space, and 3) distal movement of the upper teeth. Distal movement of the upper teeth is challenging but can be improved with temporary skeletal anchorage to move the molars backwards up to 6mm, correcting the molar relationship. For adolescents with Class II malocclusions, growth modification alone may not be enough and orthognathic surgery to advance the mandible may be necessary if little growth is expected.



































































