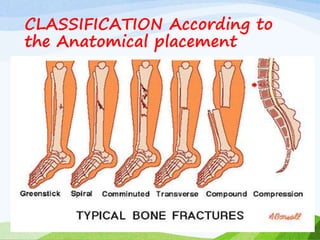
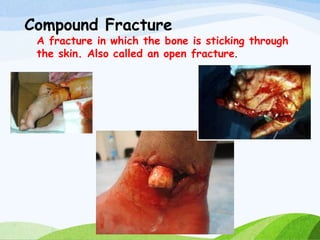
A fracture is a break in the continuity of bone that can be caused by direct blows, crushing forces, twisting motions or muscle contractions. There are two main types - complete fractures where the bone is broken across its entire cross-section, and incomplete fractures where the break is only partial. Fractures can be open (compound) if the bone protrudes through skin, or closed (simple) without skin breakage. Clinical signs include pain, deformity, swelling and loss of function. Treatment involves reduction, immobilization using casts, splints or traction, and restoring mobility while the bone heals. Complications can include nonunion, infection and compartment syndrome.