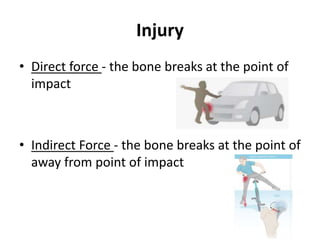
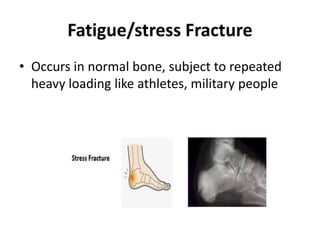
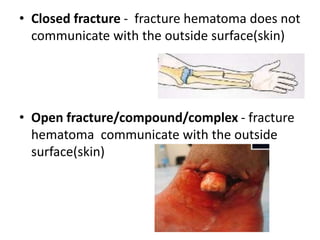
Fractures occur when bones break due to stresses that exceed the bone's strength. The causes of fractures include direct injuries, repetitive stresses, and pathological fractures caused by weakened bones from conditions like osteoporosis. Fractures are classified based on features like location, communication with the skin (open vs closed), and the direction of the break. Clinical signs include pain, swelling, deformity. Diagnosis involves history, exam, and imaging like x-rays. Treatment focuses on saving life by addressing vital organ injuries, saving the limb by splinting and assessing circulation, and saving function by properly immobilizing and rehabilitating the injury. Nursing care involves splinting, wound management, exercises, pain control, and