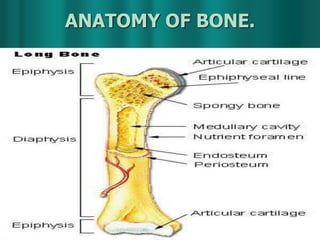
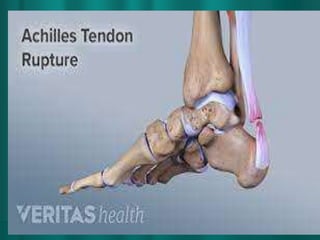
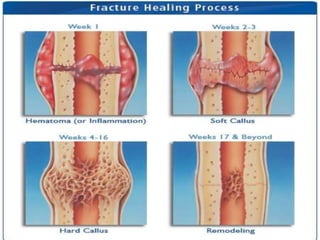
INTRODUCTION
Our skeletonis tough and flexible. It
supports weight and protects our internal
organs. Bone tissue stores minerals, such
as calcium, and it is constantly renewed,
which is how our bones are able to heal.
Bones are cleverly designed to allow
movement at the joints and provide great
stability. The bones provide a light but
strong framework for the bodies soft
tissues.
4.
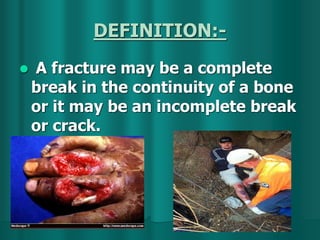
DEFINITION:-
A fracturemay be a complete
break in the continuity of a bone
or it may be an incomplete break
or crack.
• Fracture-dislocation describesjoint fractures
that produce joint instability.
This classification is incomplete, since
fracture-dislocation of the shoulder indicates
dislocation of the shoulder but does not
indicate which bone, the scapula or the
humerus, is fractured.
Fracture-dislocations can be difficult to treat
because they represent intra-articular
fracture plus supporting tissue laxity.
When fracture and dislocation are found
together, the prognosis is poorer than if each
problem occurred separately.
FRACTURE-DISLOCATION
7.
According to theiretiology ;
Fractures caused solely by sudden
injury;,
Fatigue fractures ,
Pathological fractures,
DIRECT VIOLENCE;
Trauma isthe most common cause of
fractures and is usually due to
automobile injury or falling from a
height.
Since direct trauma is rarely delivered in a
calibrated amount to a specific place,
the resultant fracture is rarely
predictable.
The amount and direction of force will
vary from accident to accident.
Most fractures resulting from violent
direct trauma are either comminuted or
multiple.
15.
INDIRECT VIOLENCE
Fracturesdue to indirect trauma are more
predictable than those due to direct
trauma.
Generally a force is transmitted to a bone
in a specific fashion and at a "weak link"
within the bone, causing a fracture to
occur.
17.
BENDING FORCES
Bendingfractures occur when force is applied to a
specific focal point on a bone to the extent that
the traumatic force overcomes the elastic limit of
the bone diaphysis.
The initial effect of a bending force is a cortical
break opposite the site of the trauma. The
periosteum will remain intact on the side of the
force while tearing over the fracture on the
opposite side.
With additional force the entire bone snaps, with
attendant tearing of vascular and soft tissue
structures within or on the diaphysis.
Bending fractures are generally oblique or
transverse, or they may have a butterfly
fragment.
19.
TORSIONAL FORCES
Torsionalfractures occur when a twisting
force is applied to the long axis of a bone.
Usually this is a result of one end of a
bone being placed in a fixed position
while the other end of the bone is forced
to rotate.
The resulting fracture will be a very long
spiral with sharp points and often sharp
edges. It is possible for the sharp points
or edges to compromise soft tissues or to
cut through the skin and result in an open
fracture. Torsional forces generally result
in short or long spiral fractures.
21.
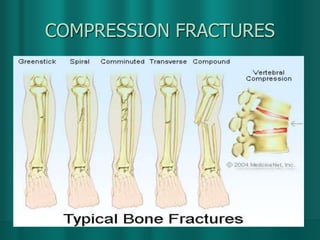
COMPRESSION FORCES
Compressiveforces along the long axis of
a bone may force the smaller diaphyseal or
metaphyseal portion of a bone to impact
into the larger epiphysis: bony substance
is thereby crushed. Similarly a
compressive force directed along the axis
of the spine may result in collapse of a
vertebral body. For compressive force to
result in fracture, one end of a bone must
be in a fixed position while the other end
is forced toward the fixed end.
Compressive forces result in impacted
fractures or compression fractures.
23.
SHEARING FORCES
Ashearing fracture is caused by a force
transmitted along the axis of a bone,
which is then transferred to a portion of
the same bone that lies peripheral to the
axis or across a joint to other bones that
are not protected by the axis of the bone.
The fracture line in a shear fracture will
be parallel to the direction of the applied
force. Shearing forces result in the
fracture of bony prominences not placed
along the direct axis of a diaphysis.
25.
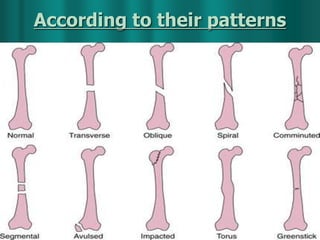
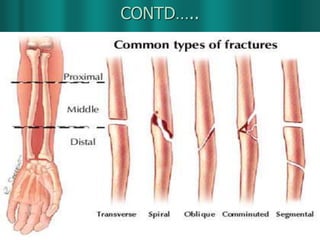
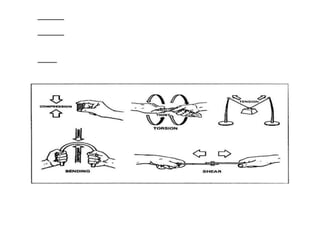
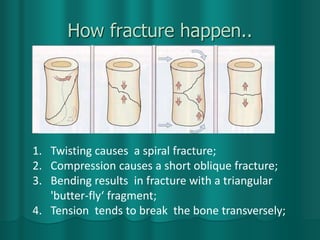
How fracture happen..
1.Twisting causes a spiral fracture;
2. Compression causes a short oblique fracture;
3. Bending results in fracture with a triangular
'butter-fly‘ fragment;
4. Tension tends to break the bone transversely;
26.
Types of Fracture…cont.
Openfracture :
When the bony fragments are
exposed to external environment by
means of wound
Closed fracture :
The fracture fragments are not
exposed to outside
FIRST AID
SEEKMEDICAL ATTENTION IMMEDIATELY. DO NOT
attempt to transport victim if you suspect head, back,
or neck injury.
Immobilize and support affected bone in position
found. DO NOT try to push protruding bone back into
body or let victim move or use affected area.
Control any bleeding through direct pressure.
If bone is protruding, cover with clean cloth once
bleeding is controlled.
Observe for shock . DO NOT give victim anything to
eat or drink.
Immobilize injured area, and, if no open wound
present, apply ice pack wrapped in clean cloth.
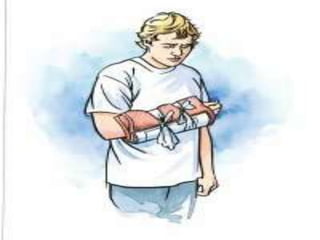
36.
Immobilizing Fractured Bone:
Check for sensation, warmth, and color of toes or
fingers below suspected break.
Place padded splint under area of suspected break.
-Use board, rolled newspaper or magazines, or
rolled blanket for splint.
-Wrap splint in cloth or towels for padding.
-Bind splint to limb using neckties, cloth, belts, or
rope. DO NOT bind directly over break.
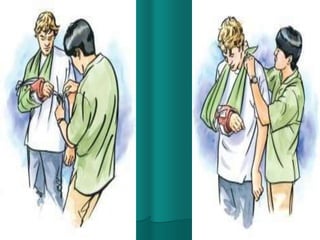
37.
CONTD…..
Recheck oftenfor sensation, warmth, and
coloring. If fingers or toes turn blue or
swell, loosen binding.
For arm or shoulder injury, place splinted
arm in sling, with hand above elbow level.
Bind arm to victim's body by wrapping
towel or cloth over sling and around upper
arm and chest; tie towel or cloth under
victim's opposite arm.
39.
Goals of fracturetreatment
Prevent fracture and soft tissue
complications,
Get fracture to heal and in satisfactory
position for optimal functional recovery.
Intra-articular fracture needs accurate
reduction & rigid fixation but non articular
fracture of bone require anatomical reduction
& stable fixation.
40.
Management of theinjured patient
Don’t treat the X-rays of the fracture, but treat
the patient
Life saving measures
Diagnose and treat life threatening injuries (head
injuries, Chest & abdominal injuries)
Emergency orthopaedic involvement
Life saving
Complication saving
Emergency orthopaedic management (day 1)
Monitoring of fracture (days to weeks)
Rehabilitation and treatment of complications
(weeks to months)
41.
Life saving measures
A= Airway and
cervical spine
immobilisation
B = Breathing
C = Circulation
(treatment and
diagnosis of cause)
D = Disability (head
injury)
E = Exposure
(musculo-skeletal
injury)
42.
Treatment principle offracture
1) Reduction
2) Maintain reduction ( hold until union)
3) Rehabilitate – restore function by movement
of the joint & patient itself.
4) Prevent or treat complications
43.
Open (compound) fractures
High risk of infection
Can be associated with gross soft tissue
damage, severe haemorrhage or vascular
injury
44.
Open (compound) fractures- management
While contacting orthopaedic team for
definitive surgical treatment
Irrigate wound with N.S, if not available with
tap water. Cover wound with sterile moist
dressing.
Immobilise limb preferable with external
fixator If not possible , by cast (including
joint above & below)
45.
CONTD…..
Remove obviouscontaminants with
meticulous effort
IV antibiotics (e.g. cefuroxime +/-
metronidazole or gentamicin)
Tetanus prophylaxis.
Check distal neurovascular status
Re-assess
46.
Reduction
If necessary,what reduction technique?
1) Closed reduction
Need anaesthesia/sedation, analgesia, x-ray
facilities, equipment, knowledge
Used for minimally displaced fractures and
most fractures of children
Distal part of limb pulled in line of bone
Alignment adjusted in each plane
2) Open reduction
Above + theatre staff + additional equipment
47.
Maintain reduction
Necessary?
1) Relievepain
2) Prevent mal-union – nature heals the
fracture, we keep it in a good position
3) Minimise non-union – maintenance of
reduction should be continuous
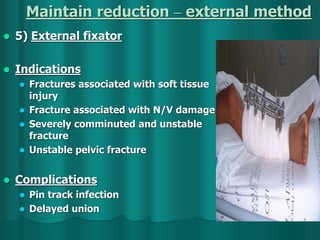
Maintain reduction –external method
1) POP
Advantages –
cheap, easy to use,
convenient, can be
moulded
Disadvantages –
susceptibility to
damage
(disintegrates when
wet), up to 48hrs to
dry
50.
Maintain reduction –external method
2) Resin cast
Advantages – lighter and
stronger, more resistant
to damage, sets in 5-
10mins, max strength in
30mins
Disadvantage – cost,
more difficult to
apply/remove, more
rigid with greater risk of
complications eg.
swelling and pressure
necrosis
51.
Maintain reduction –external method
3) Surface traction
Temporary measure
when operative
fixation not available
for awhile
Skin can be injured if
applied for long
periods of time
Neuro-vascular
status should be
checked during
surface traction
period
52.
Maintain reduction –external method
4) Skeletal traction
Requires invasive
procedure for longer
term traction requiring
heavier weights
Complications associated
with pin insertion eg.
infection
Maintain reduction –internal method
Advantages
Restoration of absolute anatomical state
Shorter hospital stay
Enables individuals to return to function
earlier
55.
Contd…..
Indications
Fracturesthat need operative fixation
Inherently unstable fractures prone to re-
displacement after reduction (eg. mid-shaft
femoral fractures)
Pathological fracture
Polytrauma (minimise ARDS)
Patients with nursing difficulties
(paraplegics, v. elderly, multiple trauma)
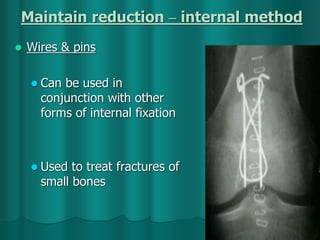
Maintain reduction –internal method
Wires & pins
Can be used in
conjunction with other
forms of internal fixation
Used to treat fractures of
small bones
58.
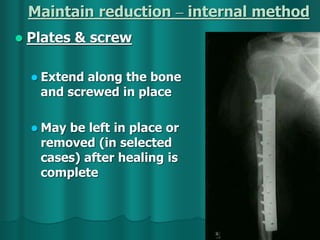
Maintain reduction –internal method
Plates & screw
Extend along the bone
and screwed in place
May be left in place or
removed (in selected
cases) after healing is
complete
59.
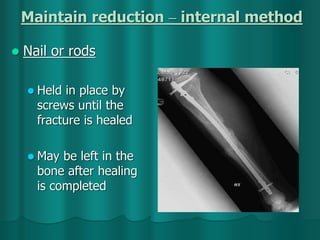
Maintain reduction –internal method
Nail or rods
Held in place by
screws until the
fracture is healed
May be left in the
bone after healing
is completed
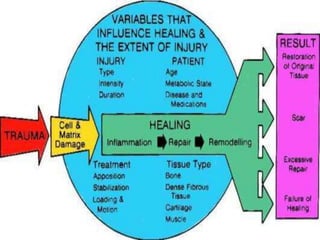
Factors Influencing Healing…cont.
LocalFactors:-
„„Energy of trauma
„„Degree of bone loss
„„Vascular injury
„„Infection
„„Type of bone fractured
„„Degree of immobilization
„„Pathological condition
65.
NURSING MANAGEMENT:-
ASSESSMENT:-
"5 P's"
Patient's general health
signs and symptoms
emotional status
understanding of need for cast
physical assessment of part to be immobilized
includes the neurovascular status of body part,
degree and location of swelling, bruising, and skin
abrasions.
66.
Cond…..
“Hot Spots”– area of the cast that feel warmer
than other sections.
May indicates tissue necrosis or infection
under the cast.
“Wet Spots” – May indicate the drainage
under the cast or a need for additional drying .
Stains can indicate wound drainage or
bleeding, any other stained area should be
measured carefully and doccumented.
67.
Contd…..
Be awareof possible pressure points on
underlying structures, such as the lateral
malleolus under a shot leg castor epicondyle
under a short arm cast.
An older cast may develop a sour smell because
of perspiration or normal sloughing of outer
skin layers.
Musty, offensive odors under the cast may
indicate tissue necrosis or infection.
If odor of mildew is present, the synthetic cast
may have not been dried properly after it
become wet
68.
CONTED…..
continuous watch forthe warning signs, which
are the ;
undue swelling
impaired circulation
severe pain within the plaster
The period of greatest danger is between 12 to
36 hours.
69.
NURSING DIAGNOSIS:-
Acute painr/t the musculoskeletal disorder.
Expected outcome:- pain in the patient's body part
will be relieved.
Nursing interventions;
Assess the characteristics of the pain. ( asking the
patient to indicate the exact site of the pain, its
severity, and intensity of the pain)
teach the diversional therapies to the patient.
70.
CONTD…..
Elevate theaffected limb.
apply the ice packs as prescribed.
restrict the unnecessary movements and
keep the body part immobilized.
involve the patient in the active and passive
ROM.
administer the analgesics as prescribed.
71.
NURSING DIAGNOSIS
Impairedskin integrity r/t lacerations
and abrasions.
Expected outcome:- skin integrity will be
maintained.
Nursing interventions;
assess for the skin of patient.
assess for the edema, redness, numbness,
parasthesia and heat.
72.
CONTD…..
elevate thebody part of the patient.
encourage for the ROM exercises.
teach about the care of the cast.
report the orthopedist, if any of
above mentioned s/s appears.
73.
NURSING DIAGNOSIS:-
Knowledge deficitr/t the treatment
regimen.
Expected outcome:- patient will obtain the optimal
level of knowledge.
Nursing interventions;
Assess the level of knowledge and
understanding of the patient.
provide the information to the patient about
the underlying pathologic condition and the
purpose and the expectations of the prescribed
treatment regimen.
74.
CONTD…..
teach the patientabout what is expected
from the patient during application.
explain about the sensations regarding
the cast application i.e. heat from the
hardening reaction of the plaster.
teach the patient that the body part will
be immobilized after the application of
the cast.
teach the about the care of the cast,
specially children.
75.
CONTD…..
Impaired physicalmobility r/t the cast.
Self care deficit : bathing/hygiene,
feeding , dressing/grooming , or
toileting due to restricted mobility.
76.
Teaching the Patientwith a Cast
Home Care:-
Mobility aids & safety
Prescribed exercise
Elevate extremity to heart level
Keep cast dry & cushion rough edges
Don’t scratch under cast
Report indicators of complications
Avoid excessive use of injured extremity
Report broken cast
77.
By-Peter F. Cronholm,MD;
Wendy Barr, MD,
Does osteoporosis screening decrease fracture risk in
postmenopausal women? Osteoporosis results in 1.3 million
fractures annually in the US. Of the approximately 25 million
American women with osteoporosis, 8 million have had a
documented fracture.
The authors reviewed articles on risk factor assessment, bone
density tests, and osteoporosis treatment with
bisphosphonates.
they found 3 clinical risk factors that consistently predicted
increased risk of fracture: advanced age, low weight or body
mass index, and nonuse of hormone replacement therapy. The
presence of any of the 3 risk factors increased the risk for
fracture by 70% (relative risk, 1.7).
Thus found that the screening of high risk women helps to
reduce the number of hip and vertebral fractures.
79.
BIBLIOGRAPHY
Black M.Joyce.MedicalSurgical Nursing(2008):Elsevier
publishers.vol-2,ed-8th. P-515 - 28
Wilkins,Williams.Mannual of Nursing
Practice(2009):Wolter Kluner.ed-9.P-279-85.
Keen Janet hicks,Swearingen Pulmelal.Critical Care
Nursing Consultant(1997):Mosby publishersvol-1st,ed-
1st.P-366,318,172,108.
Adams Jhon Crawford , Hamblen David L. Outline of
Fractures including joint injuries(1999):Churchill
Livingstone publishers, ed-11th p 1-73.
REFERENCES:-
http://cal.vet.upenn.edu/projects/saortho/chapter_1
1/11mast.htm
http://cal.vet.upenn.edu/projects/saortho/chapter_1
6/16mast.htm
../chapter_10/10mast.htm











































![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)





![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)



![APPROACH TO FEVER IN PEDIATRICS[1].pptTT](https://cdn.slidesharecdn.com/ss_thumbnails/approachtofeverinpediatrics1-260125081456-d559e079-thumbnail.jpg?width=640&height=640&fit=bounds)



