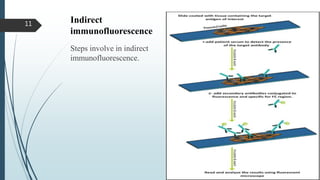
This document discusses immunofluorescence techniques used to diagnose cutaneous diseases. It describes direct, indirect, and complement indirect immunofluorescence. Direct immunofluorescence detects antigens in tissues using fluorescently-labeled antibodies. Indirect immunofluorescence detects patient antibodies using fluorescently-labeled secondary antibodies. Complement indirect immunofluorescence detects antigen-antibody complexes by binding complement proteins. Immunofluorescence is useful for detecting autoantibodies and analyzing antigen and protein distributions in tissues.