Download as PDF, PPTX


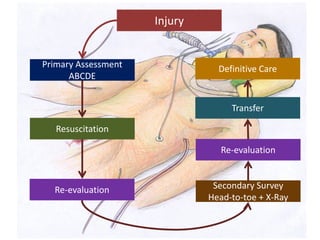
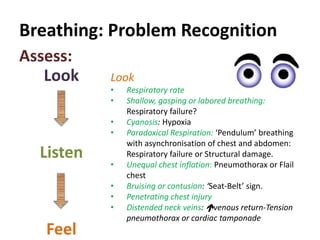
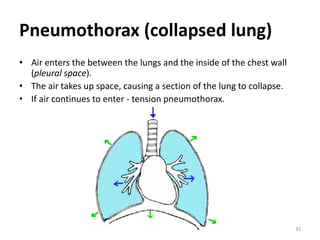
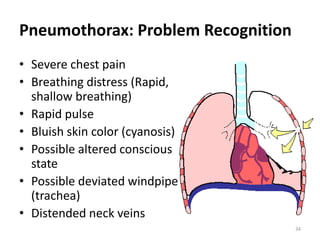
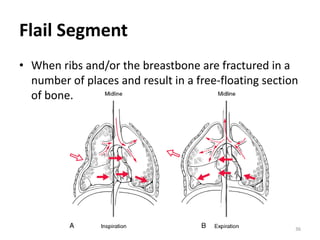
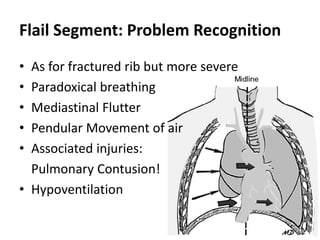


1) Chest injuries can involve external trauma, damage to internal organs like the heart and lungs, and possible spinal injury. They account for 25% of trauma-related deaths. 2) The assessment and treatment of chest injuries follows the ABCDE approach - Airway, Breathing, Circulation, Disability, Exposure. This includes treating life-threatening conditions like tension pneumothorax immediately. 3) Specific injuries like rib fractures, pneumothorax, and open chest wounds require stabilization, positioning the patient for comfort, applying dressings, and providing supplemental oxygen while seeking urgent medical care.