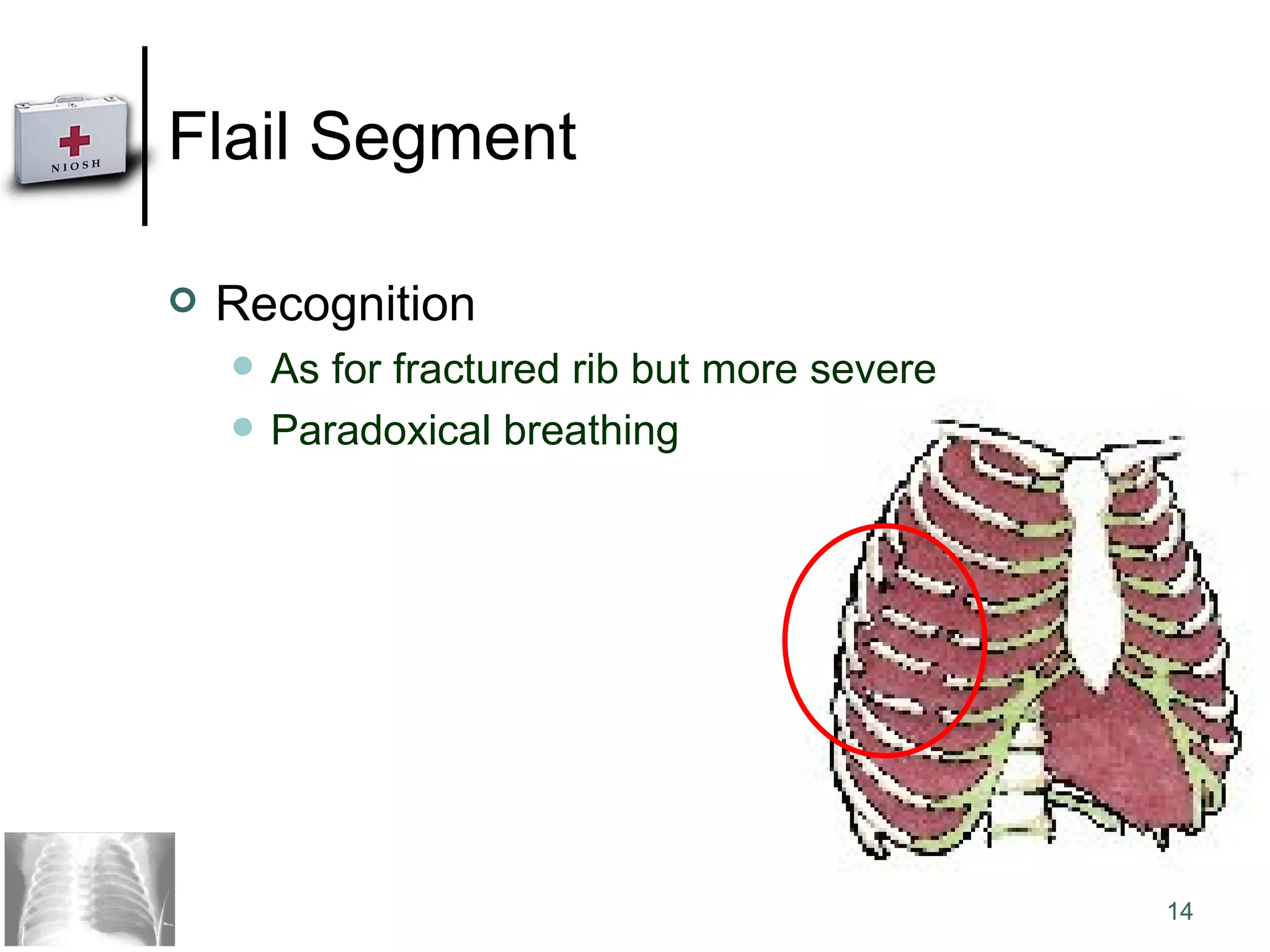
1) Chest injuries can range from fractured ribs to collapsed lungs (pneumothorax) to sections of detached rib cage (flail segment) to open chest wounds.
2) Fractured ribs are the most common chest injury and are managed by positioning the victim in comfort, stabilizing the fracture, seeking medical aid, and monitoring for breathing issues.
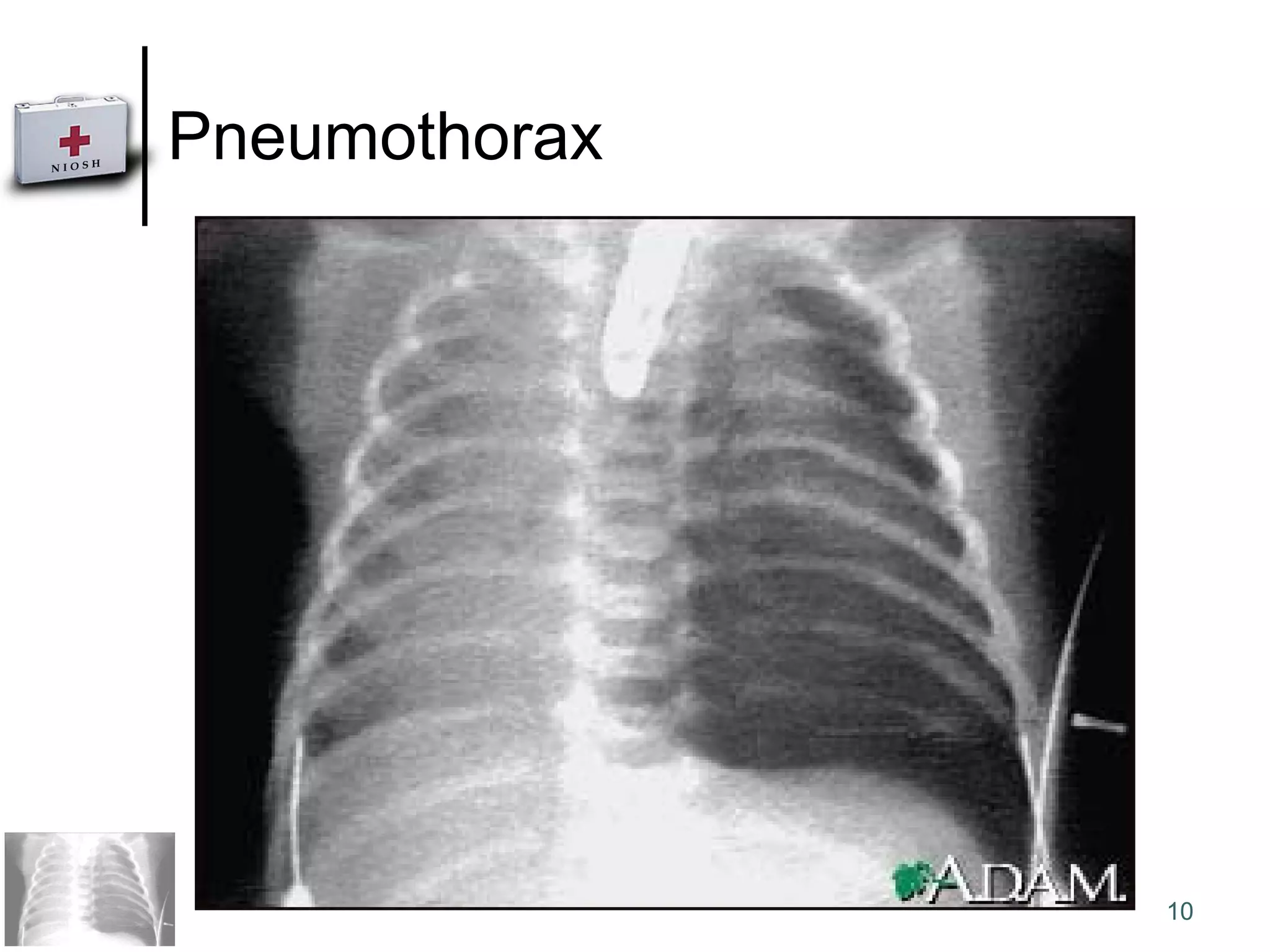
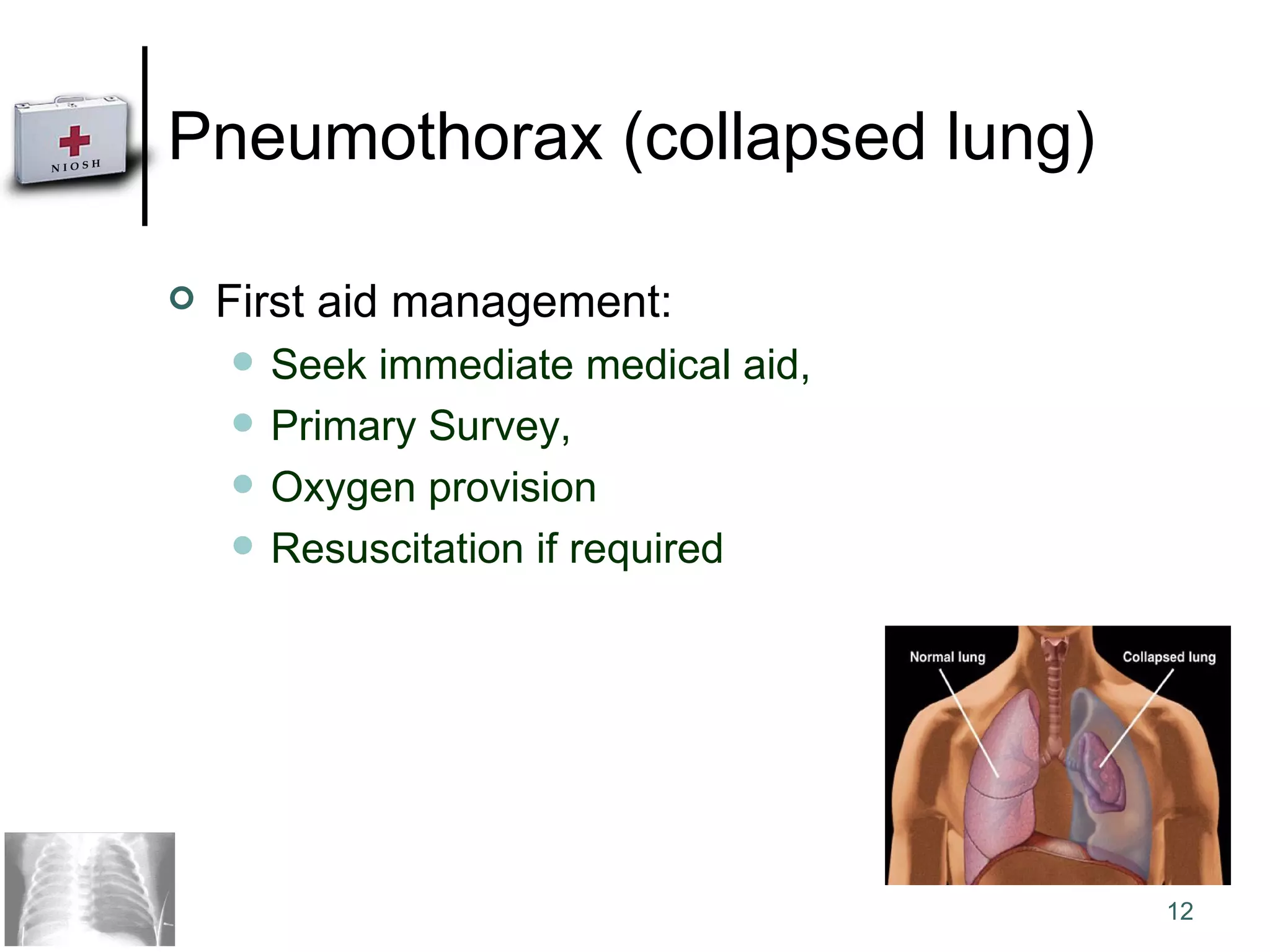
3) A collapsed lung (pneumothorax) occurs when air enters the space between the lungs and chest wall, causing pain and breathing difficulty. Immediate medical help is needed along with oxygen support.
![Chest Injuries Offshore First Aid Assoc. Prof Dr Nik Hisamuddin Nik Ab Rahman Consultant Emergency Medicine School of Medical Sciences, USM Malaysia [email_address] http://www.emergencycare.webs.com/](https://image.slidesharecdn.com/08chestinjuries-091003091552-phpapp01/75/First-Aid-For-Chest-Injury-1-2048.jpg)









































![Neuropsychiatry [2017]](https://cdn.slidesharecdn.com/ss_thumbnails/neuropsychiatricmanifestationofcommonneurologicaldisorders-171001003940-thumbnail.jpg?width=640&height=640&fit=bounds)



![Psychoses [2002]](https://cdn.slidesharecdn.com/ss_thumbnails/uupsychoses-170814005654-thumbnail.jpg?width=640&height=640&fit=bounds)







































