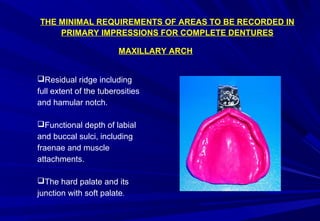
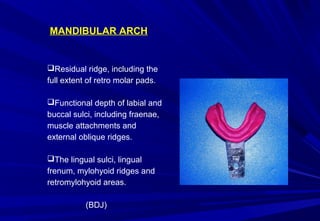
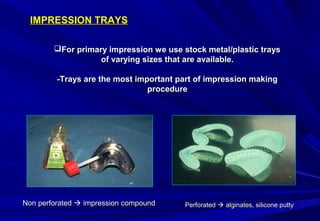
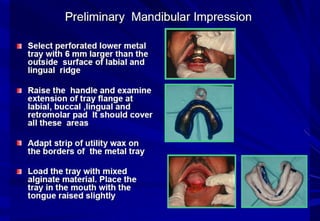
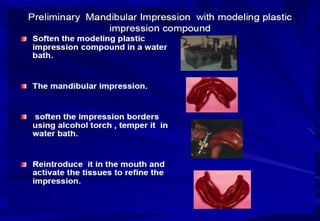


This document provides information on making complete denture impressions. It defines an impression as the negative form made of oral tissues using a plastic material. A complete denture impression captures the entire denture bearing area of an edentulous mouth. Preliminary impressions are used for diagnosis and tray construction, while final impressions make master casts for denture fabrication. Key objectives of impressions are preservation of ridges, stability, support, esthetics and retention. The document outlines techniques for primary maxillary and mandibular impressions using stock trays and high viscosity materials like alginate or impression compound. Common errors in impressions include gaps, excess material, shallow sulci and visible tray edges. Corrections involve adding material or remaking impressions.











































































































