


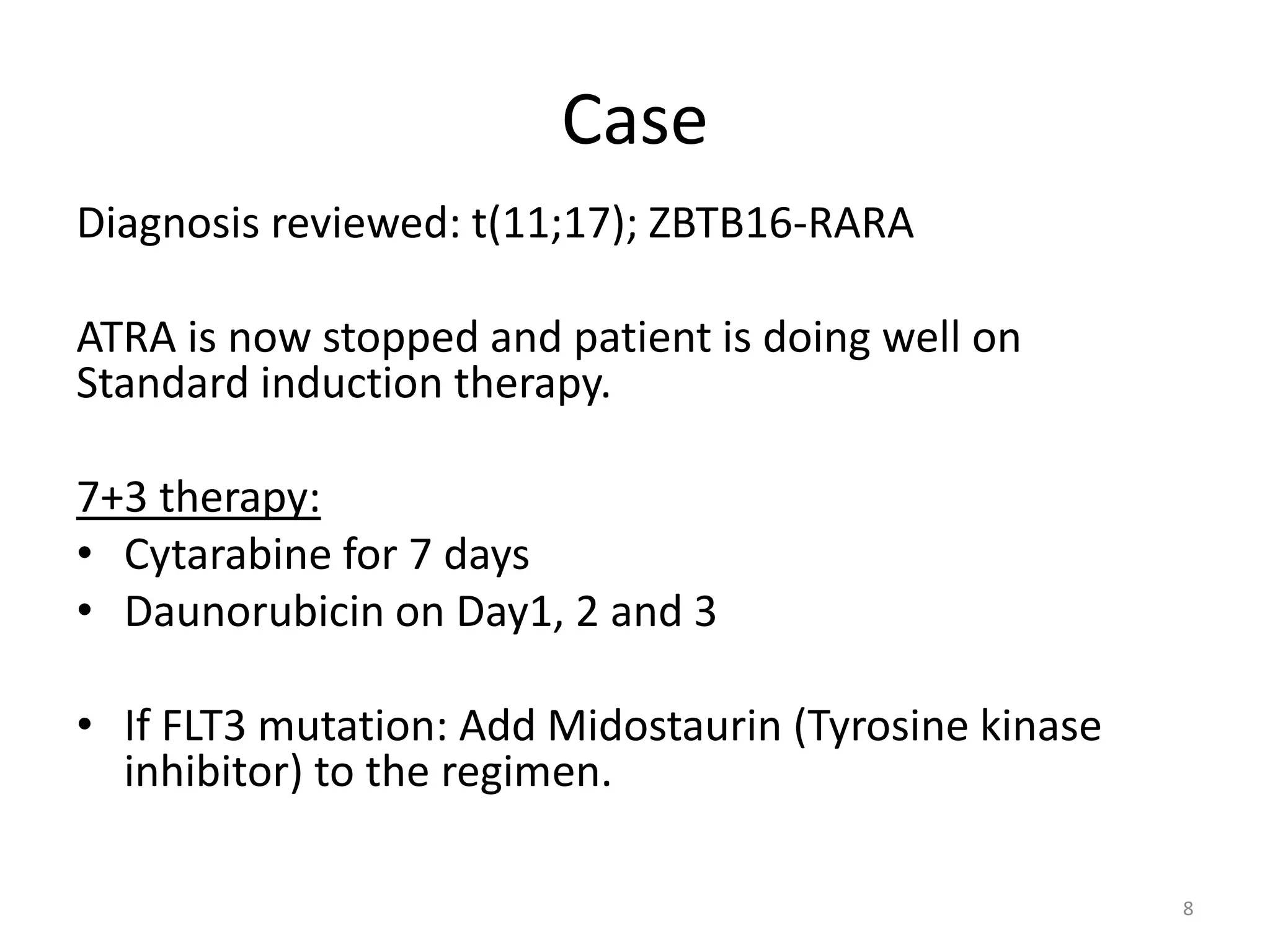



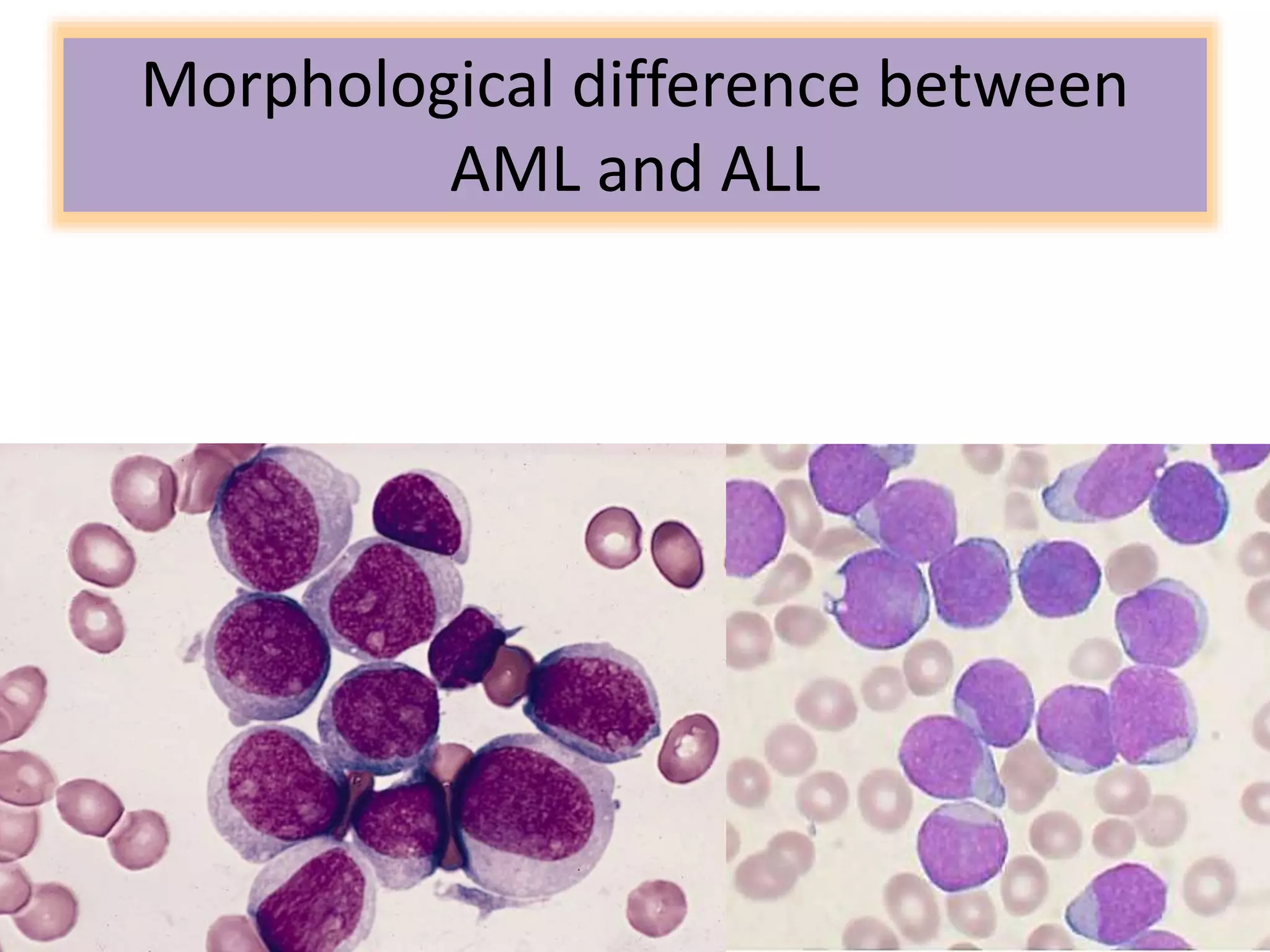
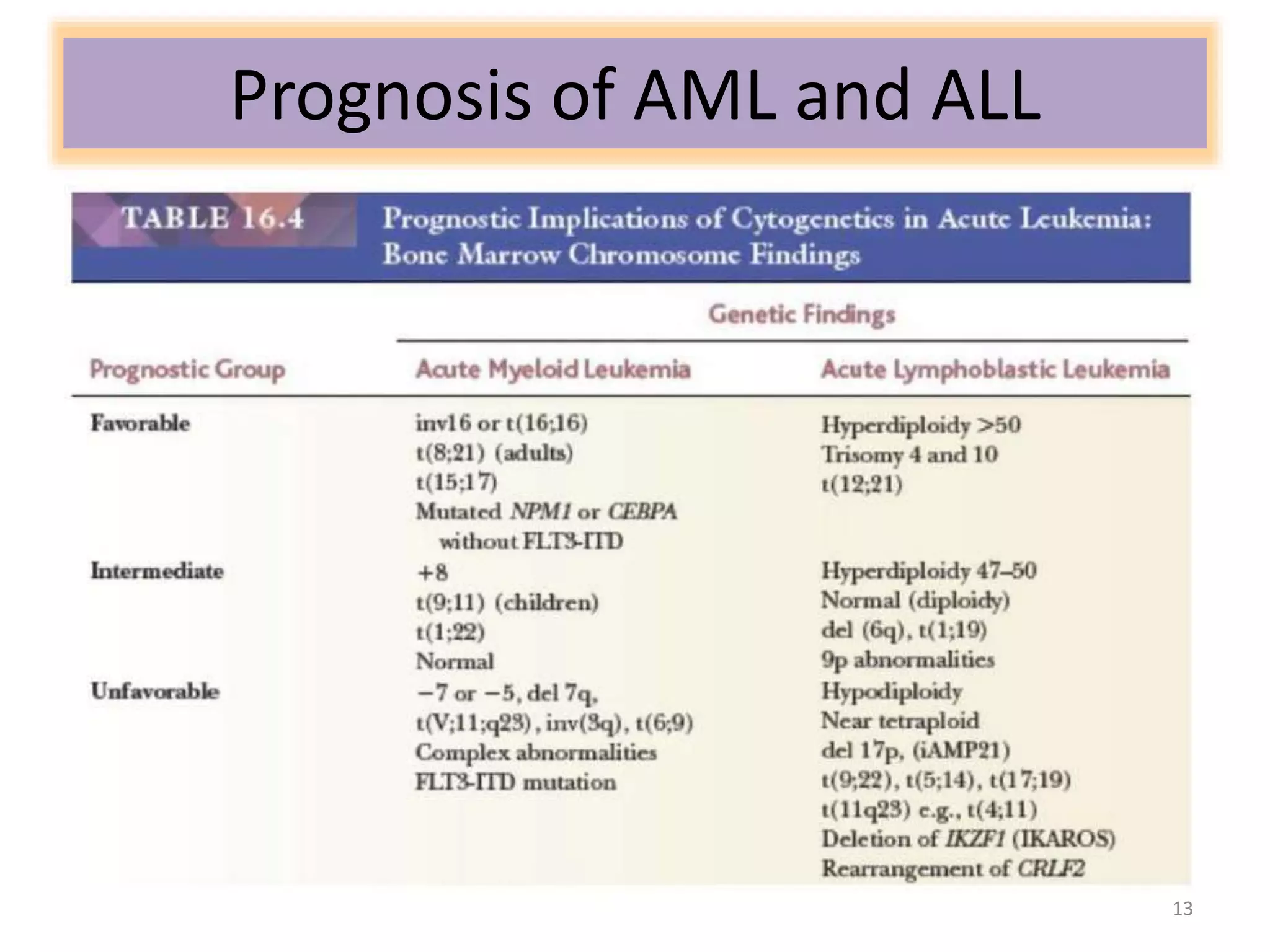


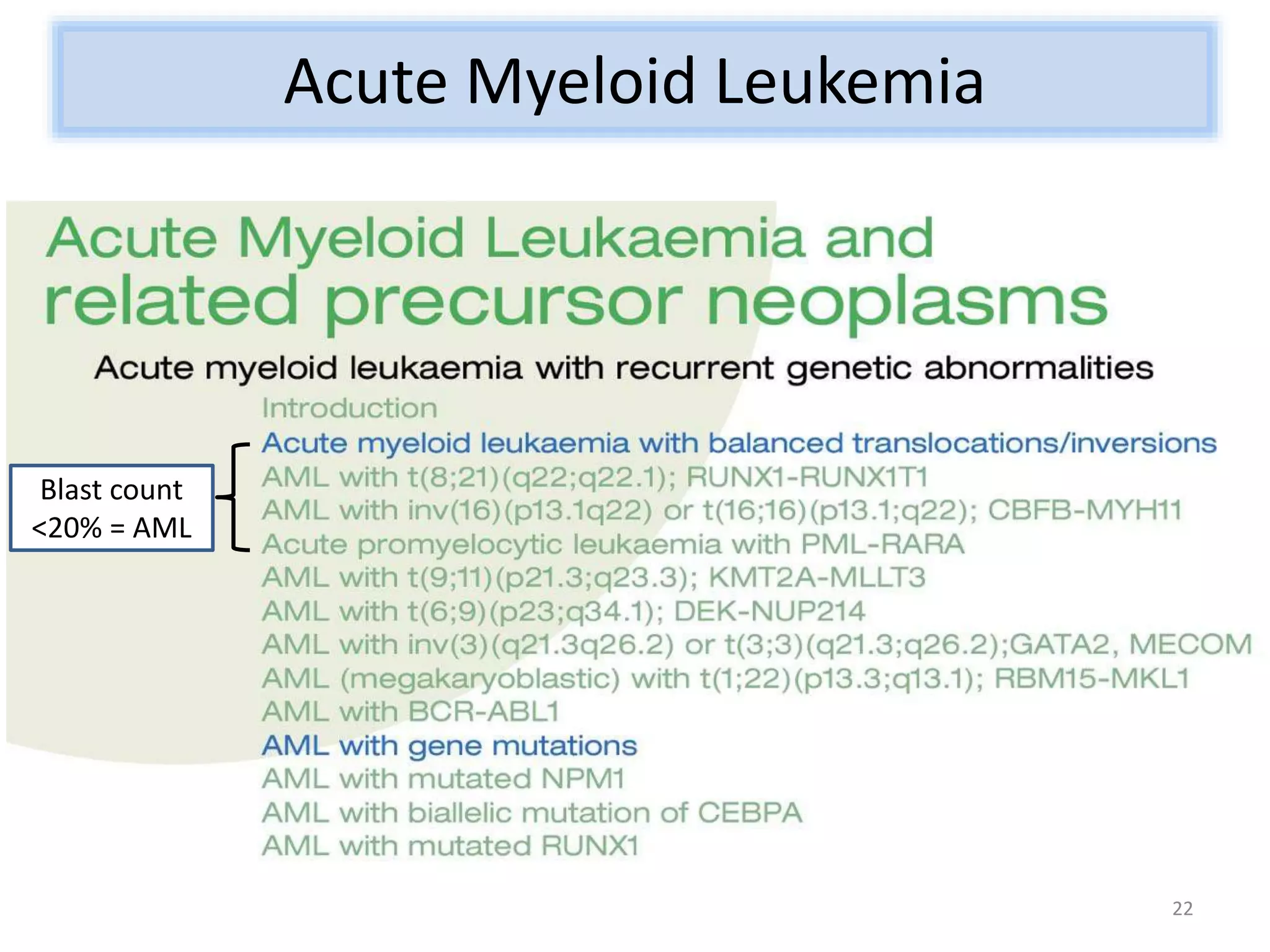

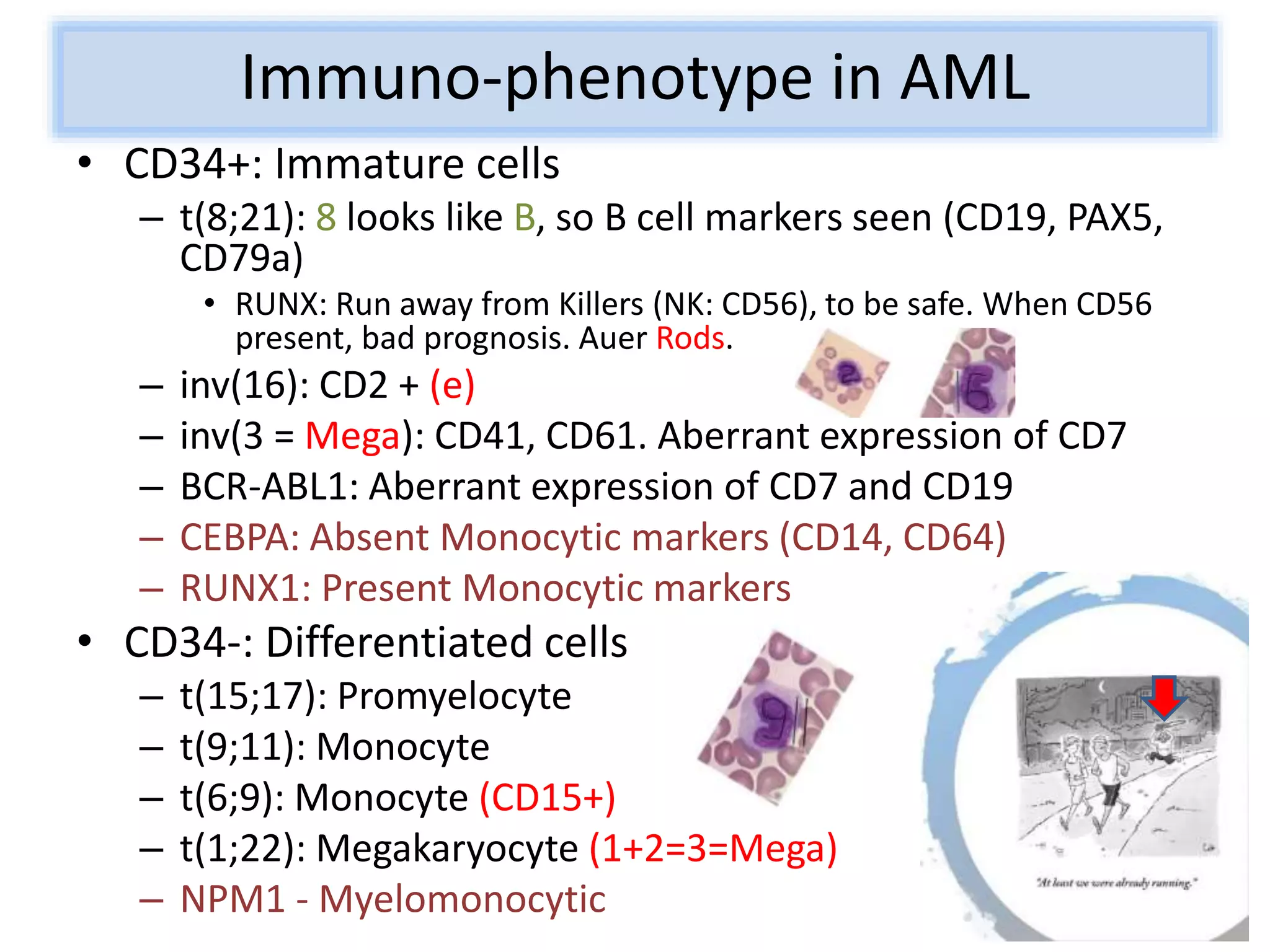
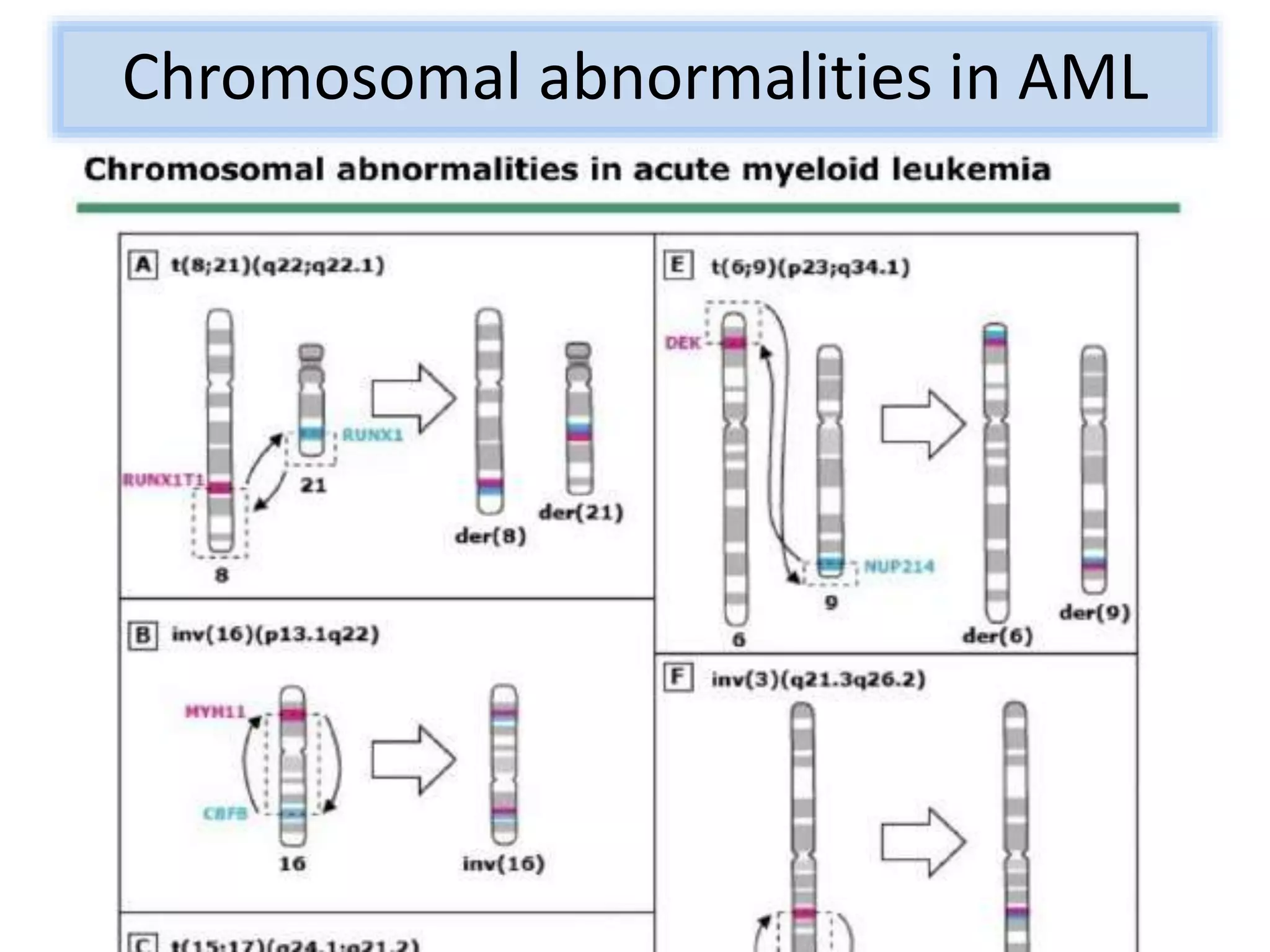

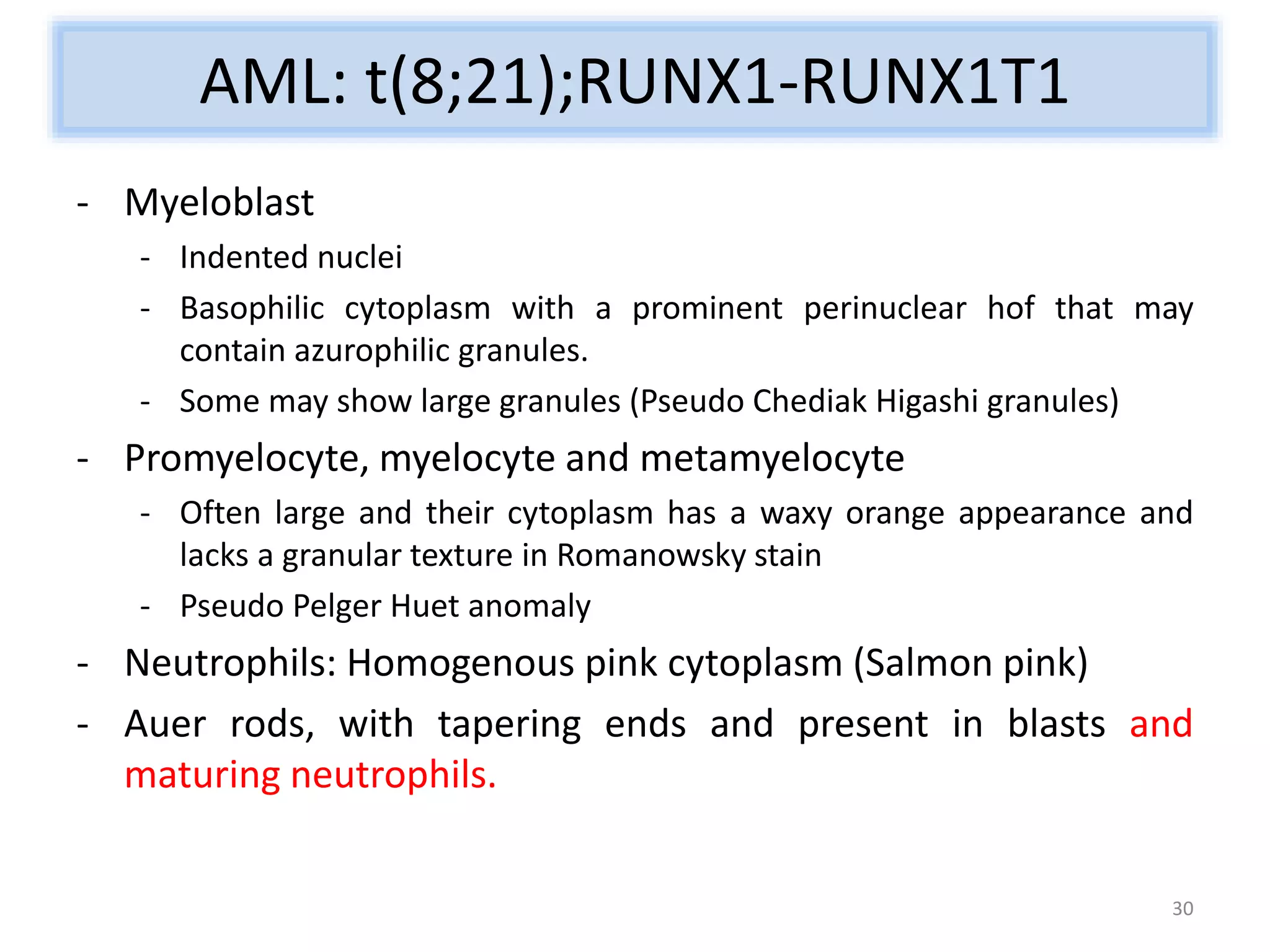

























































The document discusses various cases of Acute Myeloid Leukemia (AML) including presentations, cytogenetic findings, and treatment approaches. It emphasizes the significance of combining morphologic, immuno-phenotypic, cytogenetic, and molecular studies for accurate diagnosis and differentiation of AML variants. Multiple case studies illustrate unique markers, translocations, and therapy responses related to different AML subtypes.


















































































