Downloaded 495 times






![Intussusception
Intussusception is a process in which a segment of intestine invaginates into the adjoining
intestinal lumen, causing bowel obstruction.
A common cause of abdominal pain in children, intussusception is suggested readily in pediatric
practice based on a classic triad of signs and symptoms: vomiting, abdominal pain, and
passage of blood per rectum.
Intussusception presents in 2 variants:
A. Idiopathic intussusception, which usually starts at the ileocolic junction and affects
infants and toddlers .
B. Enteroenteral intussusception (jejunojejunal, jejunoileal, ileoileal), which occurs
in older children. associated with special medical situations (eg, Henoch-Schönlein
purpura [HSP], cystic fibrosis, hematologic dyscrasias) or may be secondary to a lead
point and occasionally occur in the postoperative period.](https://image.slidesharecdn.com/acuteabdomeninchildren-150305140037-conversion-gate01/85/Acute-abdomen-in-children-36-320.jpg)



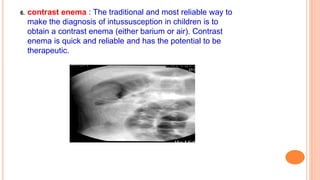

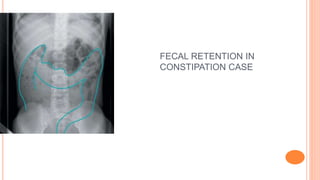



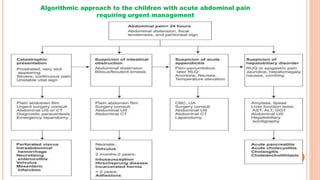
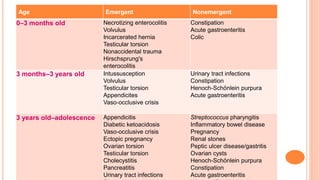
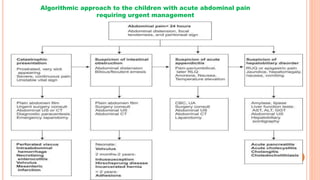
The document discusses the evaluation and management of acute abdominal pain in children, highlighting the importance of timely diagnosis to prevent severe complications. It covers common causes such as appendicitis, gastroenteritis, and intussusception, and emphasizes the need for careful clinical evaluation, including history taking and physical examination. The management strategies include addressing underlying causes, supportive care, and potential surgical intervention when necessary.



































































