The face receives its blood supply from the facial artery and transverse facial arteries which accompany cutaneous nerves. The facial vein drains venous blood from the face. It forms from the union of other veins and drains into the internal jugular vein. The facial nerve provides motor innervation to the muscles of facial expression while the trigeminal nerve provides sensory innervation. The lymphatic drainage of the face occurs through preauricular, submandibular and submental lymph nodes.
The ear is the organ of hearing and, in mammals, balance. In mammals, the ear is usually described as having three parts the outer ear, the middle ear and the inner ear. The outer ear consists of the pinna and the ear canal.
The human face is a fascinating study of physiology and psychology. Face is the mirror of one’s personality. It is our most useful and most underestimated tool for communication.
Face is the most beautiful and attractive part of the body which is most likely to develop malformations. So, the knowledge of normal anatomy of face will aid in understanding the potential reasons for preventing or treating of anomalies.
The ear is the organ of hearing and, in mammals, balance. In mammals, the ear is usually described as having three parts the outer ear, the middle ear and the inner ear. The outer ear consists of the pinna and the ear canal.
The human face is a fascinating study of physiology and psychology. Face is the mirror of one’s personality. It is our most useful and most underestimated tool for communication.
Face is the most beautiful and attractive part of the body which is most likely to develop malformations. So, the knowledge of normal anatomy of face will aid in understanding the potential reasons for preventing or treating of anomalies.
Neurovascular topography of the face and neckEric Jewell
Anatomy presentation on the neurovascular topography of the face and neck. DOWNLOAD TO SEE THE COMMENTS. The slides are very basic - most of the info is contained in the comments which I read during the presentation.
Report Back from SGO 2024: What’s the Latest in Cervical Cancer?bkling
Are you curious about what’s new in cervical cancer research or unsure what the findings mean? Join Dr. Emily Ko, a gynecologic oncologist at Penn Medicine, to learn about the latest updates from the Society of Gynecologic Oncology (SGO) 2024 Annual Meeting on Women’s Cancer. Dr. Ko will discuss what the research presented at the conference means for you and answer your questions about the new developments.
- Video recording of this lecture in English language: https://youtu.be/lK81BzxMqdo
- Video recording of this lecture in Arabic language: https://youtu.be/Ve4P0COk9OI
- Link to download the book free: https://nephrotube.blogspot.com/p/nephrotube-nephrology-books.html
- Link to NephroTube website: www.NephroTube.com
- Link to NephroTube social media accounts: https://nephrotube.blogspot.com/p/join-nephrotube-on-social-media.html
These lecture slides, by Dr Sidra Arshad, offer a quick overview of physiological basis of a normal electrocardiogram.
Learning objectives:
1. Define an electrocardiogram (ECG) and electrocardiography
2. Describe how dipoles generated by the heart produce the waveforms of the ECG
3. Describe the components of a normal electrocardiogram of a typical bipolar leads (limb II)
4. Differentiate between intervals and segments
5. Enlist some common indications for obtaining an ECG
Study Resources:
1. Chapter 11, Guyton and Hall Textbook of Medical Physiology, 14th edition
2. Chapter 9, Human Physiology - From Cells to Systems, Lauralee Sherwood, 9th edition
3. Chapter 29, Ganong’s Review of Medical Physiology, 26th edition
4. Electrocardiogram, StatPearls - https://www.ncbi.nlm.nih.gov/books/NBK549803/
5. ECG in Medical Practice by ABM Abdullah, 4th edition
6. ECG Basics, http://www.nataliescasebook.com/tag/e-c-g-basics
micro teaching on communication m.sc nursing.pdfAnurag Sharma
Microteaching is a unique model of practice teaching. It is a viable instrument for the. desired change in the teaching behavior or the behavior potential which, in specified types of real. classroom situations, tends to facilitate the achievement of specified types of objectives.
Anti ulcer drugs and their Advance pharmacology ||
Anti-ulcer drugs are medications used to prevent and treat ulcers in the stomach and upper part of the small intestine (duodenal ulcers). These ulcers are often caused by an imbalance between stomach acid and the mucosal lining, which protects the stomach lining.
||Scope: Overview of various classes of anti-ulcer drugs, their mechanisms of action, indications, side effects, and clinical considerations.
Factory Supply Best Quality Pmk Oil CAS 28578–16–7 PMK Powder in Stockrebeccabio
Factory Supply Best Quality Pmk Oil CAS 28578–16–7 PMK Powder in Stock
Telegram: bmksupplier
signal: +85264872720
threema: TUD4A6YC
You can contact me on Telegram or Threema
Communicate promptly and reply
Free of customs clearance, Double Clearance 100% pass delivery to USA, Canada, Spain, Germany, Netherland, Poland, Italy, Sweden, UK, Czech Republic, Australia, Mexico, Russia, Ukraine, Kazakhstan.Door to door service
Hot Selling Organic intermediates
The prostate is an exocrine gland of the male mammalian reproductive system
It is a walnut-sized gland that forms part of the male reproductive system and is located in front of the rectum and just below the urinary bladder
Function is to store and secrete a clear, slightly alkaline fluid that constitutes 10-30% of the volume of the seminal fluid that along with the spermatozoa, constitutes semen
A healthy human prostate measures (4cm-vertical, by 3cm-horizontal, 2cm ant-post ).
It surrounds the urethra just below the urinary bladder. It has anterior, median, posterior and two lateral lobes
It’s work is regulated by androgens which are responsible for male sex characteristics
Generalised disease of the prostate due to hormonal derangement which leads to non malignant enlargement of the gland (increase in the number of epithelial cells and stromal tissue)to cause compression of the urethra leading to symptoms (LUTS
Lung Cancer: Artificial Intelligence, Synergetics, Complex System Analysis, S...Oleg Kshivets
RESULTS: Overall life span (LS) was 2252.1±1742.5 days and cumulative 5-year survival (5YS) reached 73.2%, 10 years – 64.8%, 20 years – 42.5%. 513 LCP lived more than 5 years (LS=3124.6±1525.6 days), 148 LCP – more than 10 years (LS=5054.4±1504.1 days).199 LCP died because of LC (LS=562.7±374.5 days). 5YS of LCP after bi/lobectomies was significantly superior in comparison with LCP after pneumonectomies (78.1% vs.63.7%, P=0.00001 by log-rank test). AT significantly improved 5YS (66.3% vs. 34.8%) (P=0.00000 by log-rank test) only for LCP with N1-2. Cox modeling displayed that 5YS of LCP significantly depended on: phase transition (PT) early-invasive LC in terms of synergetics, PT N0—N12, cell ratio factors (ratio between cancer cells- CC and blood cells subpopulations), G1-3, histology, glucose, AT, blood cell circuit, prothrombin index, heparin tolerance, recalcification time (P=0.000-0.038). Neural networks, genetic algorithm selection and bootstrap simulation revealed relationships between 5YS and PT early-invasive LC (rank=1), PT N0—N12 (rank=2), thrombocytes/CC (3), erythrocytes/CC (4), eosinophils/CC (5), healthy cells/CC (6), lymphocytes/CC (7), segmented neutrophils/CC (8), stick neutrophils/CC (9), monocytes/CC (10); leucocytes/CC (11). Correct prediction of 5YS was 100% by neural networks computing (area under ROC curve=1.0; error=0.0).
CONCLUSIONS: 5YS of LCP after radical procedures significantly depended on: 1) PT early-invasive cancer; 2) PT N0--N12; 3) cell ratio factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) LC characteristics; 9) LC cell dynamics; 10) surgery type: lobectomy/pneumonectomy; 11) anthropometric data. Optimal diagnosis and treatment strategies for LC are: 1) screening and early detection of LC; 2) availability of experienced thoracic surgeons because of complexity of radical procedures; 3) aggressive en block surgery and adequate lymph node dissection for completeness; 4) precise prediction; 5) adjuvant chemoimmunoradiotherapy for LCP with unfavorable prognosis.
ARTIFICIAL INTELLIGENCE IN HEALTHCARE.pdfAnujkumaranit
Artificial intelligence (AI) refers to the simulation of human intelligence processes by machines, especially computer systems. It encompasses tasks such as learning, reasoning, problem-solving, perception, and language understanding. AI technologies are revolutionizing various fields, from healthcare to finance, by enabling machines to perform tasks that typically require human intelligence.
Title: Sense of Smell
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the primary categories of smells and the concept of odor blindness.
Explain the structure and location of the olfactory membrane and mucosa, including the types and roles of cells involved in olfaction.
Describe the pathway and mechanisms of olfactory signal transmission from the olfactory receptors to the brain.
Illustrate the biochemical cascade triggered by odorant binding to olfactory receptors, including the role of G-proteins and second messengers in generating an action potential.
Identify different types of olfactory disorders such as anosmia, hyposmia, hyperosmia, and dysosmia, including their potential causes.
Key Topics:
Olfactory Genes:
3% of the human genome accounts for olfactory genes.
400 genes for odorant receptors.
Olfactory Membrane:
Located in the superior part of the nasal cavity.
Medially: Folds downward along the superior septum.
Laterally: Folds over the superior turbinate and upper surface of the middle turbinate.
Total surface area: 5-10 square centimeters.
Olfactory Mucosa:
Olfactory Cells: Bipolar nerve cells derived from the CNS (100 million), with 4-25 olfactory cilia per cell.
Sustentacular Cells: Produce mucus and maintain ionic and molecular environment.
Basal Cells: Replace worn-out olfactory cells with an average lifespan of 1-2 months.
Bowman’s Gland: Secretes mucus.
Stimulation of Olfactory Cells:
Odorant dissolves in mucus and attaches to receptors on olfactory cilia.
Involves a cascade effect through G-proteins and second messengers, leading to depolarization and action potential generation in the olfactory nerve.
Quality of a Good Odorant:
Small (3-20 Carbon atoms), volatile, water-soluble, and lipid-soluble.
Facilitated by odorant-binding proteins in mucus.
Membrane Potential and Action Potential:
Resting membrane potential: -55mV.
Action potential frequency in the olfactory nerve increases with odorant strength.
Adaptation Towards the Sense of Smell:
Rapid adaptation within the first second, with further slow adaptation.
Psychological adaptation greater than receptor adaptation, involving feedback inhibition from the central nervous system.
Primary Sensations of Smell:
Camphoraceous, Musky, Floral, Pepperminty, Ethereal, Pungent, Putrid.
Odor Detection Threshold:
Examples: Hydrogen sulfide (0.0005 ppm), Methyl-mercaptan (0.002 ppm).
Some toxic substances are odorless at lethal concentrations.
Characteristics of Smell:
Odor blindness for single substances due to lack of appropriate receptor protein.
Behavioral and emotional influences of smell.
Transmission of Olfactory Signals:
From olfactory cells to glomeruli in the olfactory bulb, involving lateral inhibition.
Primitive, less old, and new olfactory systems with different path
Surgical Site Infections, pathophysiology, and prevention.pptx
Facenervevessels dr.Meher
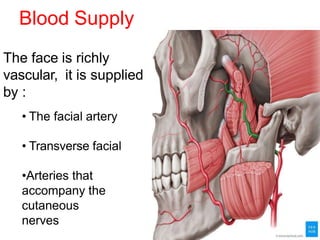
1. Blood Supply
The face is richly
vascular, it is supplied
by :
• The facial artery
• Transverse facial
•Arteries that
accompany the
cutaneous
nerves
2. Facial Artery
It is chief artery of
face It is branch of
external carotid
artery
Two parts of facial
artery-
1.Cervical part- runs
downwards in the
neck
3. Branches of facial part
1. Inferior labial –
- supplies lower lip
2. Superior labial-
- supplies the upper
lip & the anteroinferior
part of the nasal septum.
3. Lateral nasal-
- supplies to the ala
& dorsum of the nose.
4. Transverse facial
Branch of superficial
temporal artery.
•After emerging from the parotid
gland, it runs forward over the
masseter between the parotid duct
& zygomatic arch.
•Accompanied by the upper
buccal branch of facial nerve.
•It supplies the parotid gland & its
duct
,the masseter & overlying skin.
5. Venous Drainage of Face
The venous blood from the face is
drained by two veins-
1. Facial vein
2. Retromandibular vein
Facial Vein
Formation- it is the largest vein
of the face
• At the medial angle of the eye
by the union of supratrochlear
and supraorbital veins,
angular vein is formed.
6. e
o
• Course- The angular
vein continues as the
facial vein , running
downwards and
backwards behind the
facial artery ,but with a
straighter course at
anteroinferior angl of
masseter.
• Here it pierces the deep
fasia, crosses superficial
to submandibular
gland and joins the
anterior division of
retromandibular vein
below the angle of the
mandible to form the
common facial vein,
which drains into the
internal jugular vein.
7. The facial vein
communicates with the
cavernous sinus
through the two routes:-
1. A communication between
the supraorbital and
superior ophthalmic vein.
2. Connection with the
pterygoid plexus through
the deep facial vein which
passes backward over the
buccinator
Facial vain – Deep facial vein
–pterygoid venous plexus–
Emissary vein –cavernous
sinus
8. Dangerous area of face
• Infection from face can spread in a retrograde direction and
cause thrombosis of the cavernous sinus.
• This is specially likely to occur in the presence of infection in the
upper lip
and in the lower part of the nose, this is known as dangerous area of
face.
• facial vein is connected to cavernous sinus through superior
ophthalmic vein & it provides a pathway for spread of infection from
face to cavernous sinus.
9. NERVE
SUPPLY
Each half of face
has
Sensory
Branches of
Trigeminal
Nerve 5th
cranial nerve
Motor
Branches
of Facial
nerve
7th cranial
nerve
10. Sensory
supplyCutaneous innervation of the face is by
Trigeminal nerve
Areas supplied :
-Ophthalmic zone includes tip and side of
the nose, upper eye lid and forehead
-Maxillary zone upper lip, part of the side
of nose, lower eye lid, cheeks and small
part of temple
-Mandibular zone include lower chin, skin
overlying mandible, part of pinna, external
acoustic meatus and temple
12. Facial
Nerve (Motor
supply)
It emerges from
stylomastoid foramen to
enter the parotid gland , it
supplies all muscles of
facial expression except
masseter.
Stylomastoid
Foramen
13. It runs within
substance of
parotid gland, it
divides into 5
terminal branches :
• Temporal- frontalis, auricular
muscles, orbicularis oculi
• Zygomatic- orbicularis
oculi
• Buccal – muscles of cheek and
upper lip
• Mandibular –muscles
Of lower lip
• Cervical -
platysma
Temporal
Zygomatic
Buccal
Mandibular
Cervical
14. Clinical
aspect
Infranuclear lesion
Also known as Bell’s Palsy
Clinical features :
• Whole face of the same side gets
paralysed.
• Face becomes asymmetrical
• Face drawn up to normal side
• Affected side is motionless
• Wrinkles disappear from the forehead
• Eye cannot be closed
• Any attempt to smile draws the mouth
to normal side
• During mastication ,food
accumulates between teeth and
cheek
• Articulation of labials is impaired.
15. Supra nuclear lesion
•They are usually
part of hemiplegia
•Only lower part of
opposite side of face
is paralysed
•Upper part of
frontalis and
orbicularis oculi
escapes
•due to its bilateral
representation in the
cerebral cortex
16. Lymphatic Drainage of the
Face
The face has 3 lymphatic territories-
1. Upper territory- Preauricular (parotid)
nodes
Including:
• The greater part of the forehead
• Lateral halves of the eylids
• The conjunctiva
• Lateral part of the cheek
• Parotid area
17. Middle territory-
Submandibular
nodes
• Median part of the
forehead
• External nose
• Upper lip
• Lateral part of lower lip
• Medial halves of eyelids
• Medial part of cheek
• Greater part of the lower
jaw
It may involve one or more division of trigeminal nerve
It causes attack of very severe burning and scalding pain along the distribution of the affected nerve
Pain is relieved either :
By injecting 90% alcohol into the affected division of trigeminal ganglion
By sectioning the affected nerve, the main sensory root,or the spinal tract of trigeminal nerve which is situated superficially in medulla so the procedure is known as Medullary Tractotomy