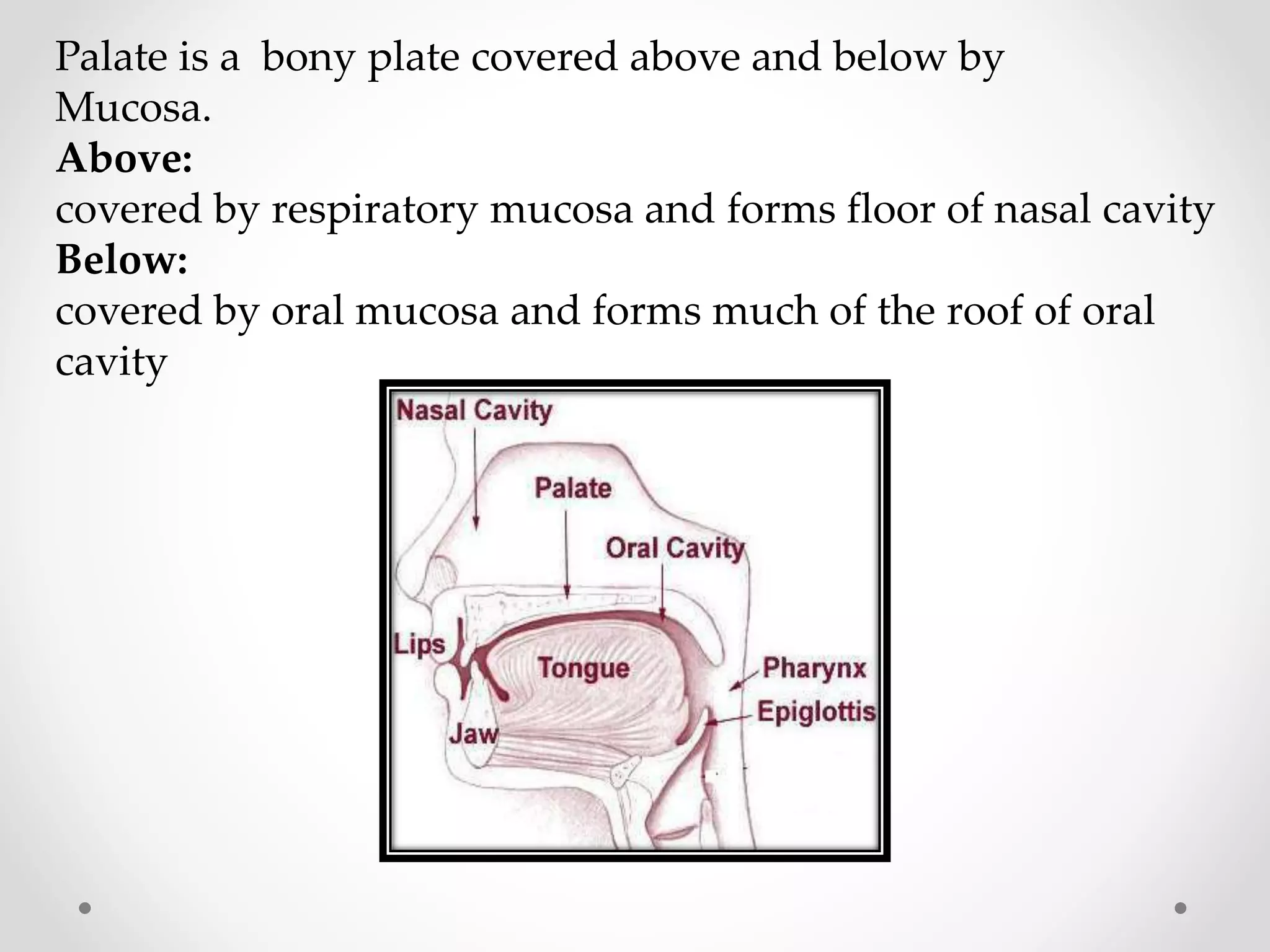
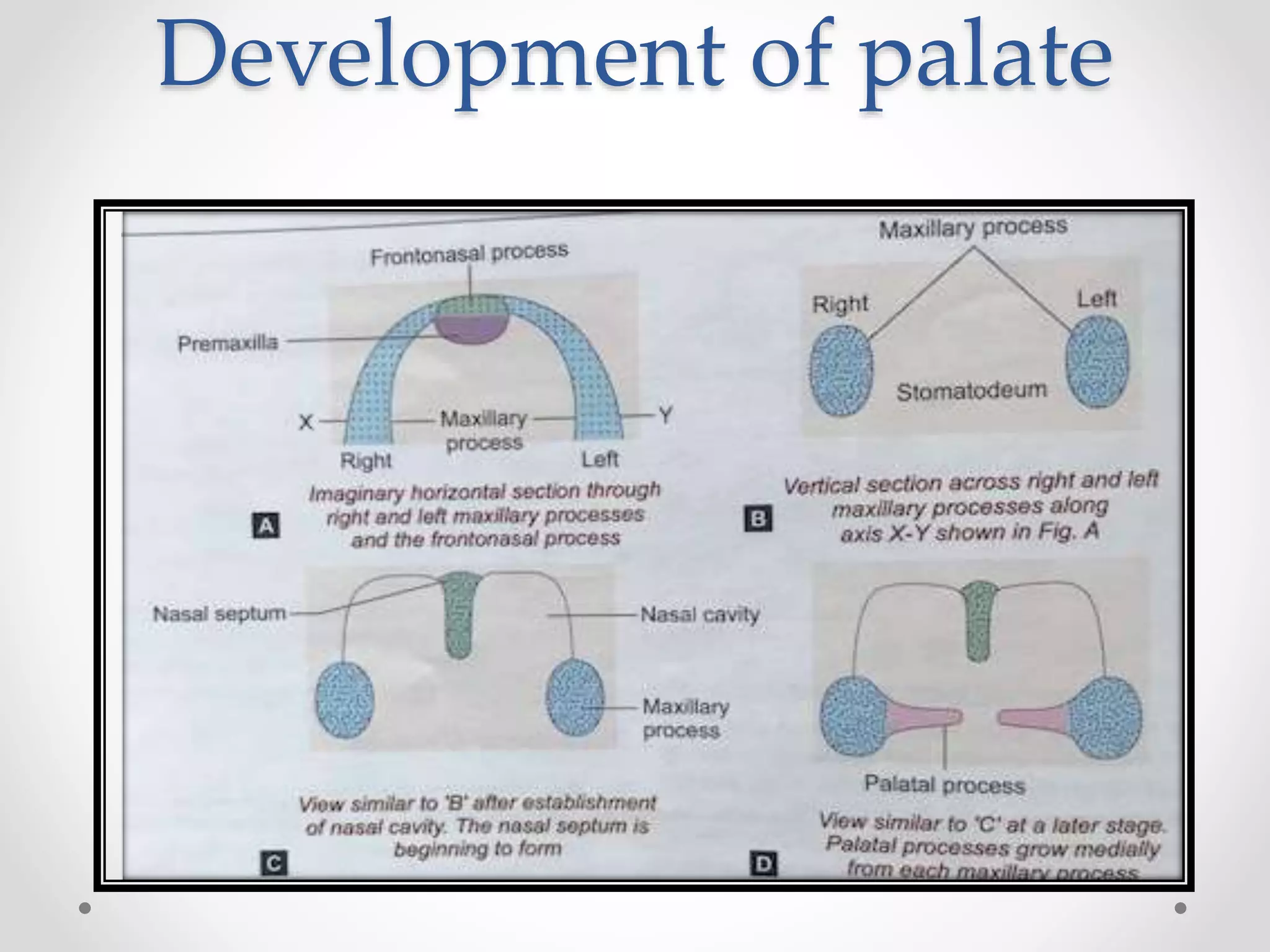
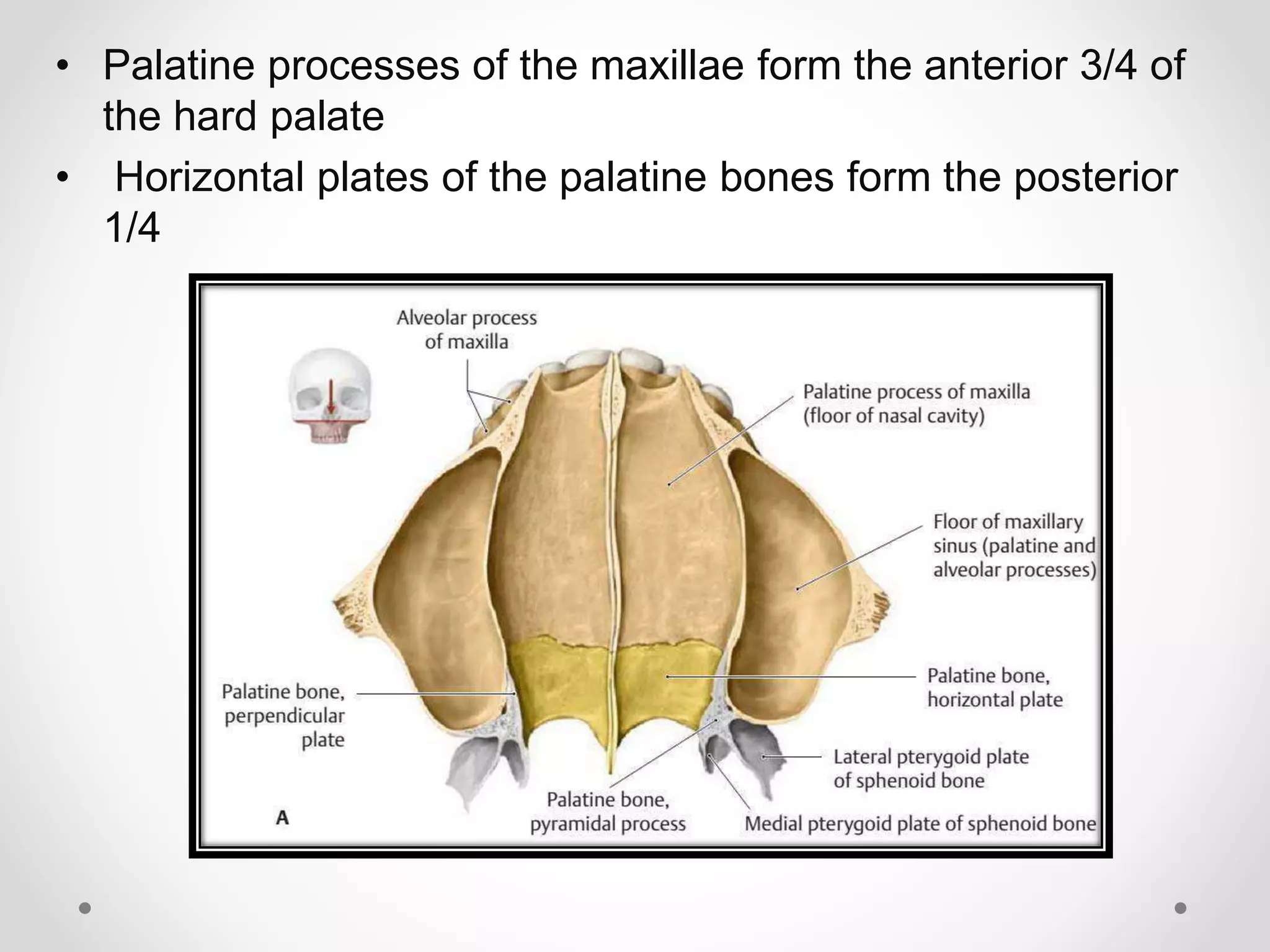
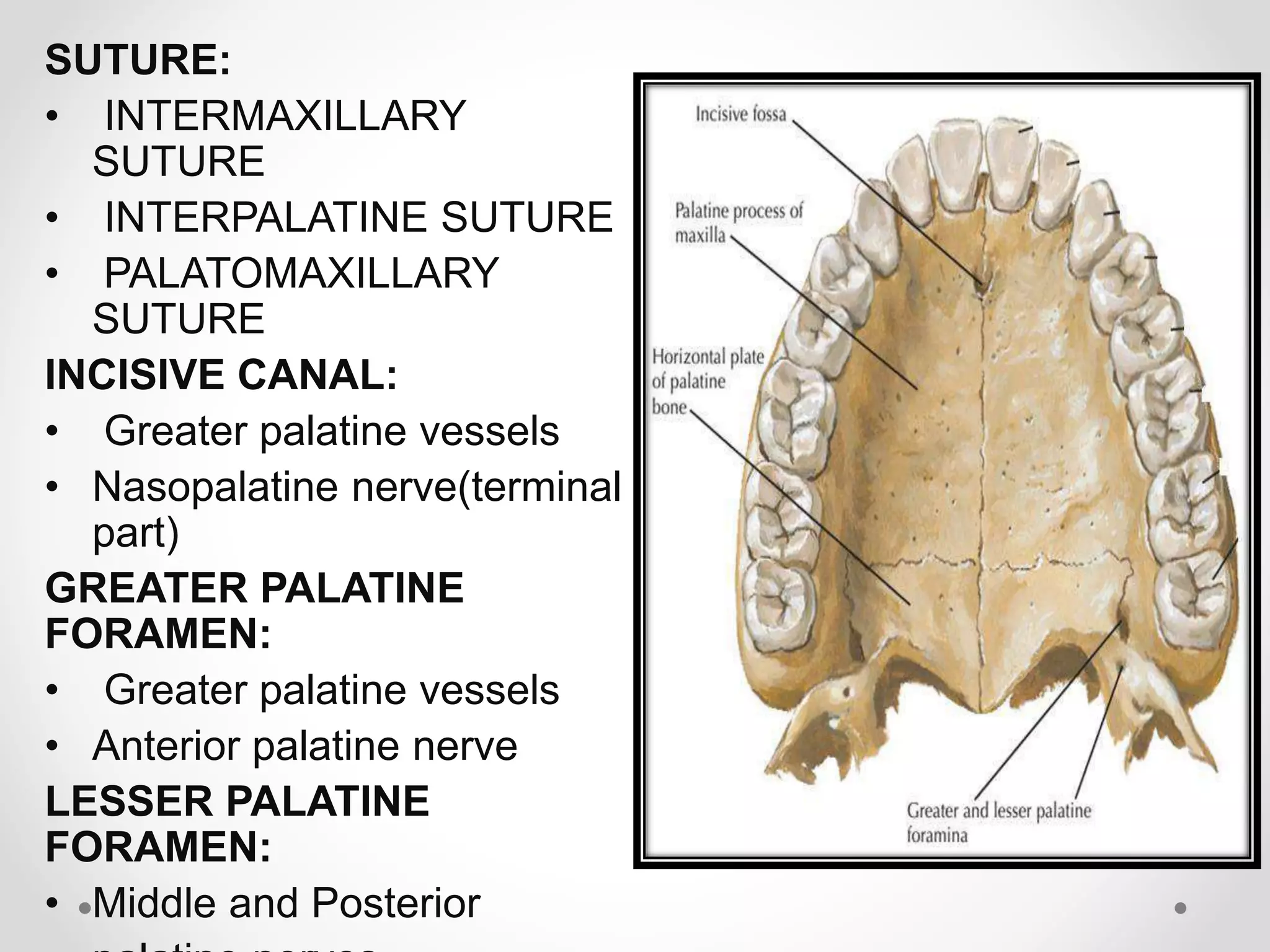
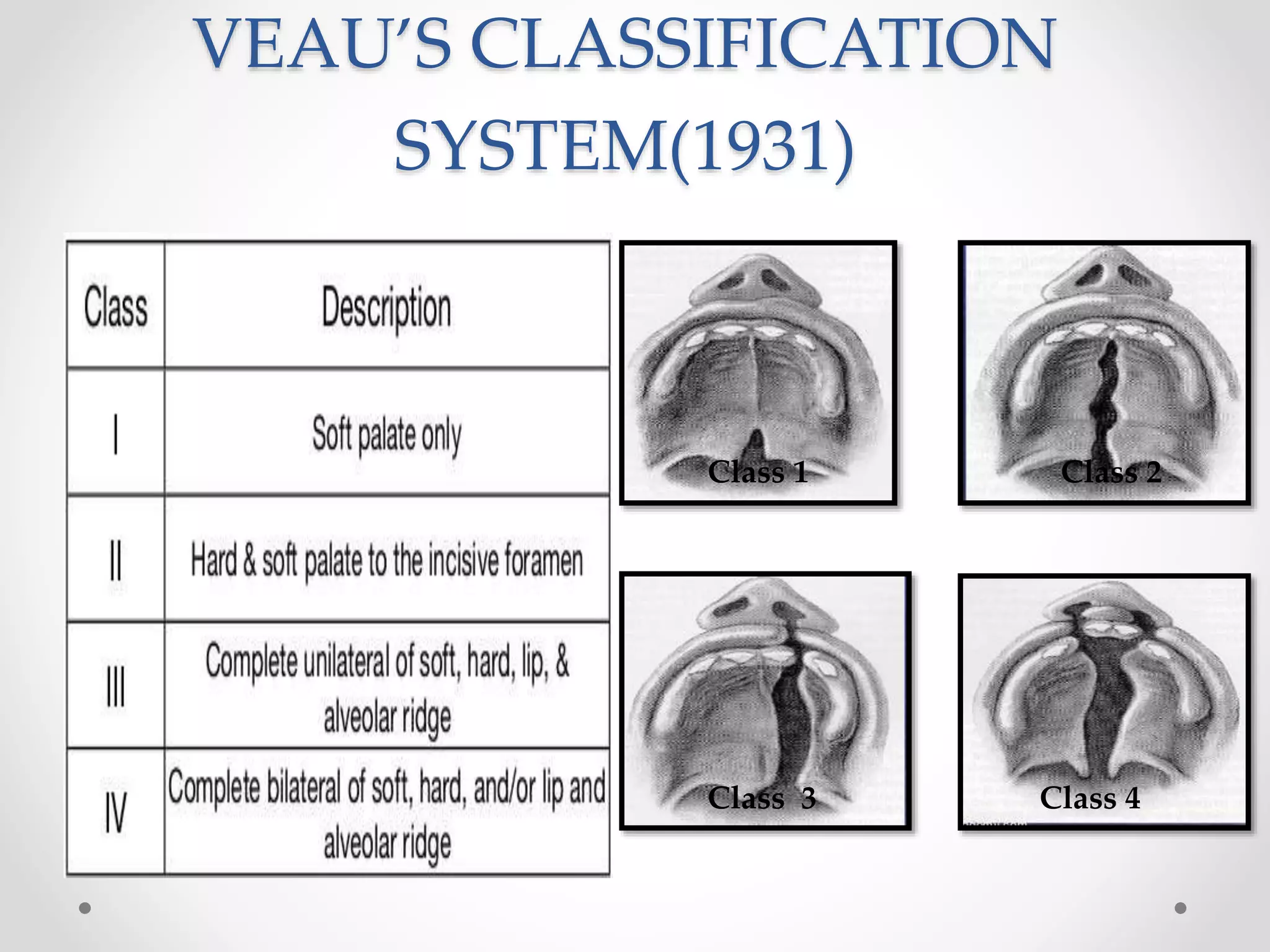
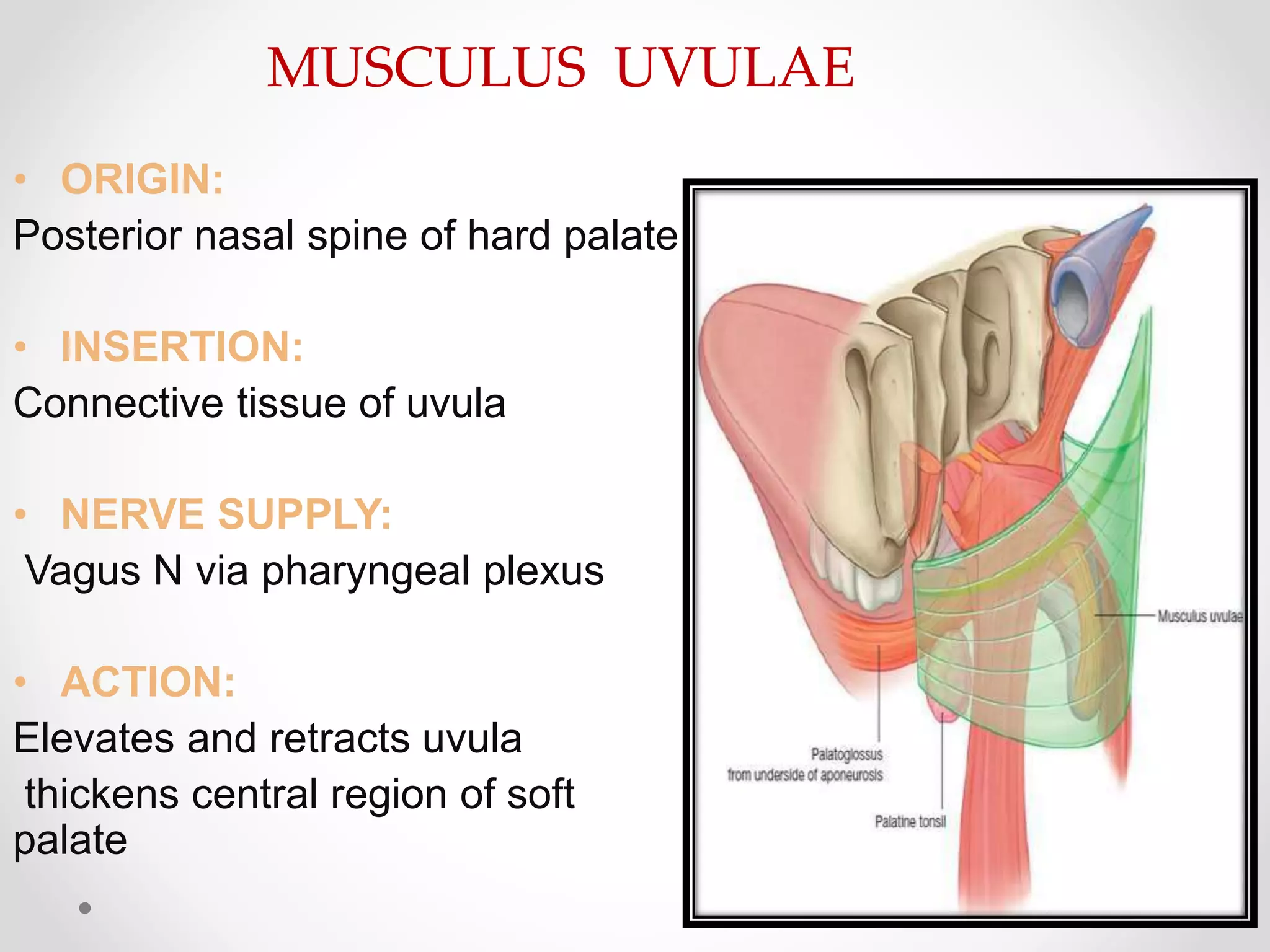
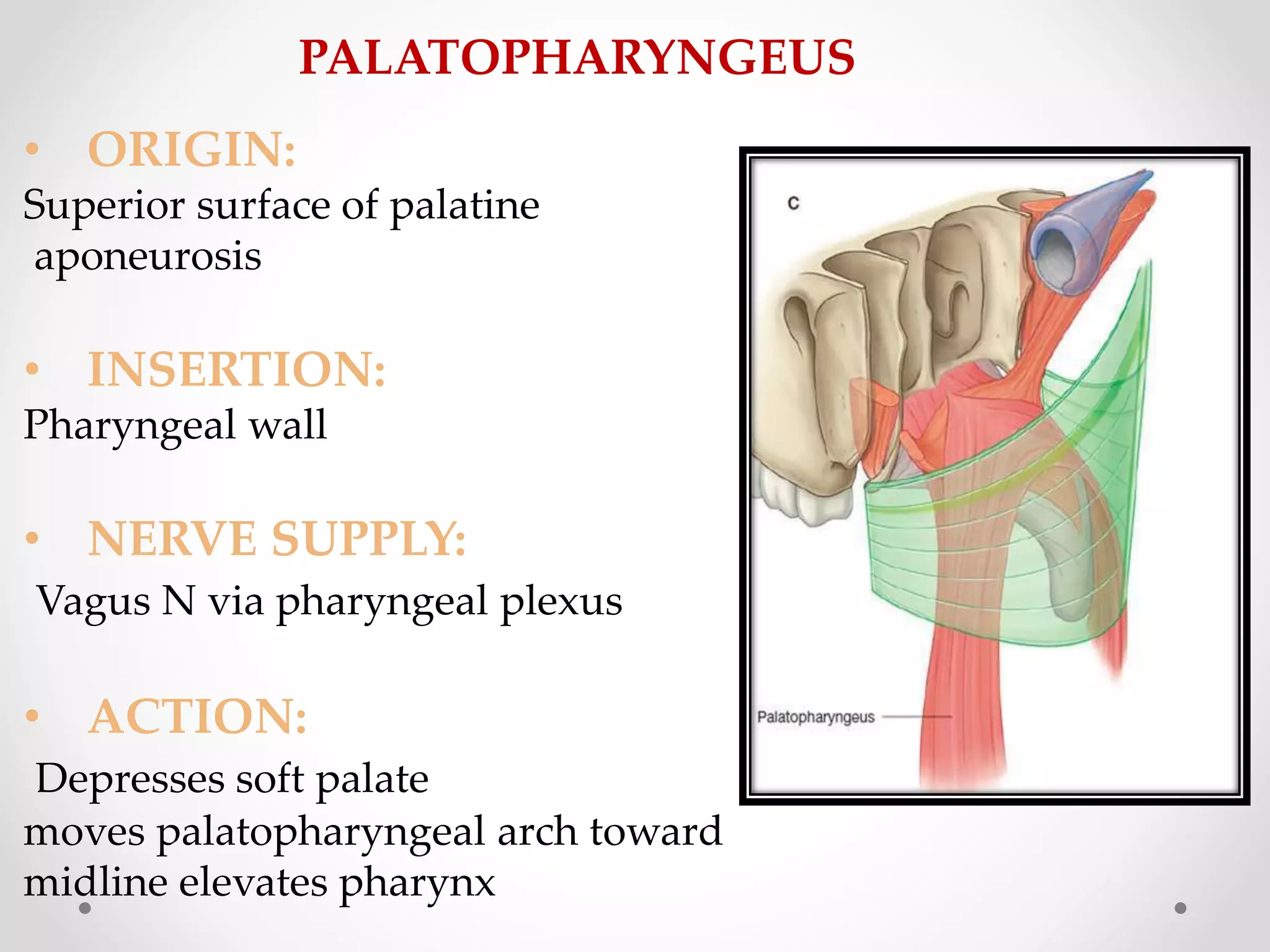
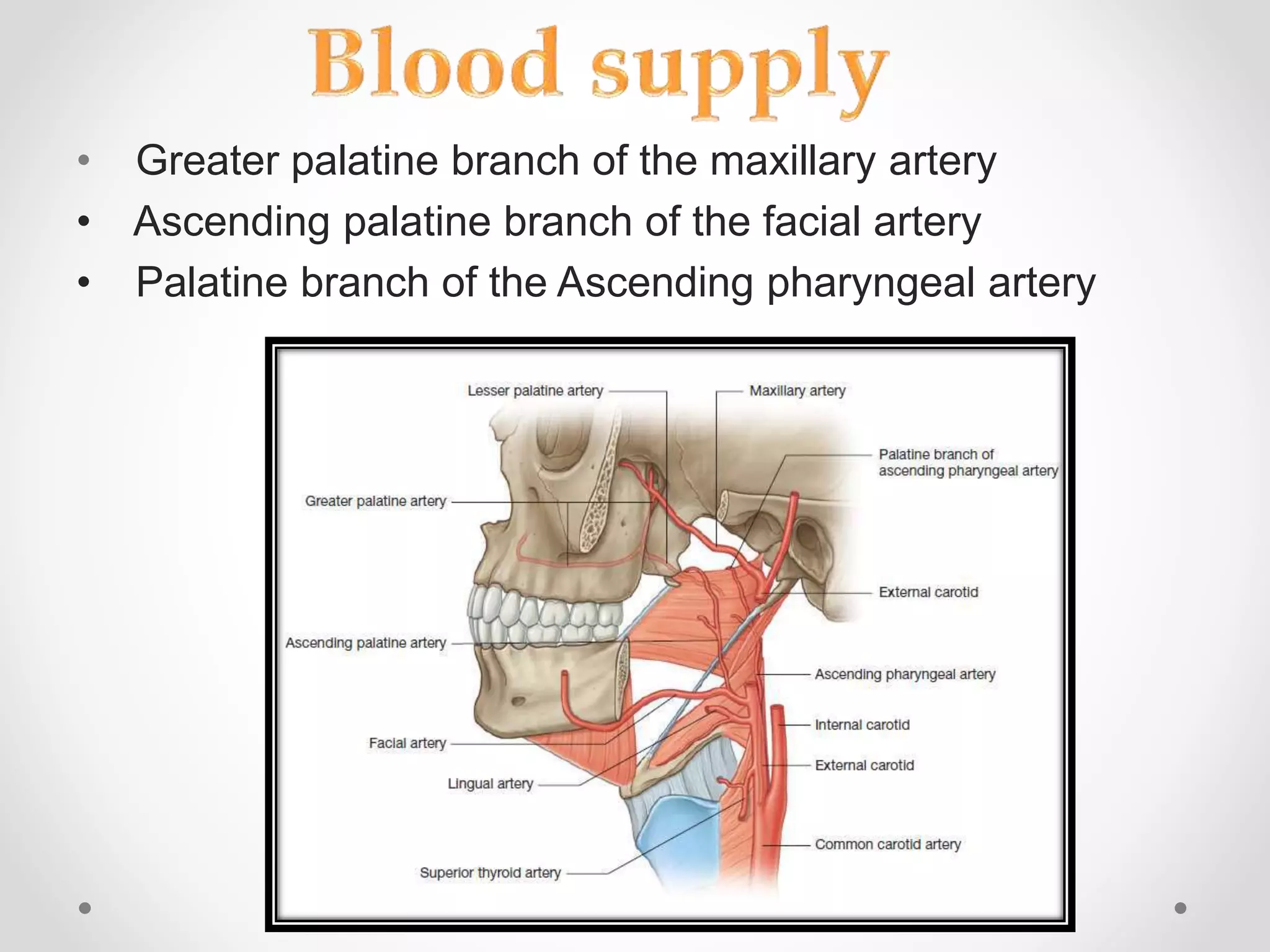
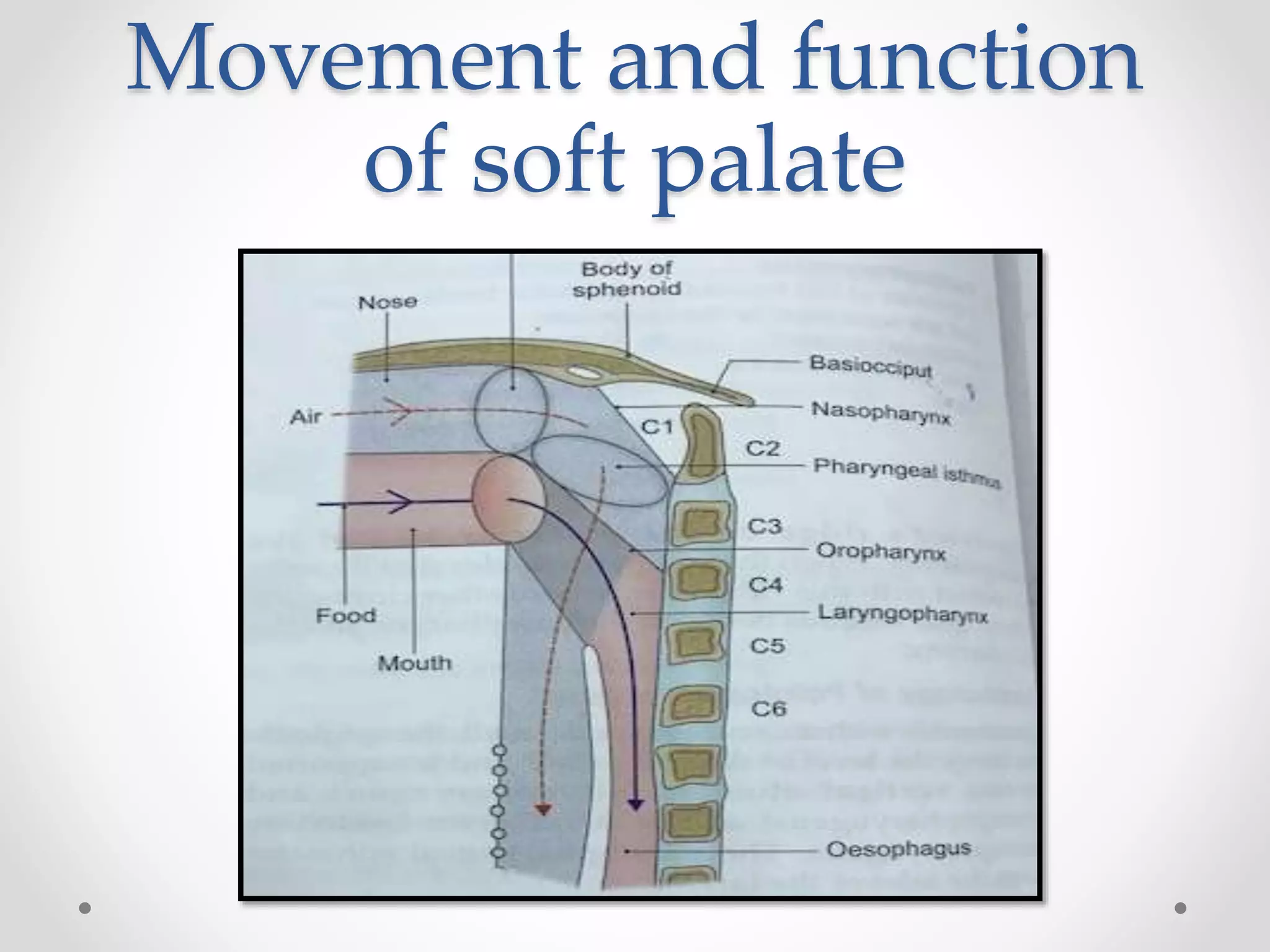
The document discusses the anatomy, development, and prosthodontic considerations of the hard and soft palate. It begins with an introduction to the palate and its two parts: the anterior hard palate and posterior soft palate. It then covers the embryological development of the palate and anatomical structures of both parts such as bones, muscles, nerves and vessels. Developmental anomalies including various cleft classifications are discussed. Finally, the document addresses prosthodontic factors related to different palate types and tissues that are important to consider for denture construction and retention.