Downloaded 78 times





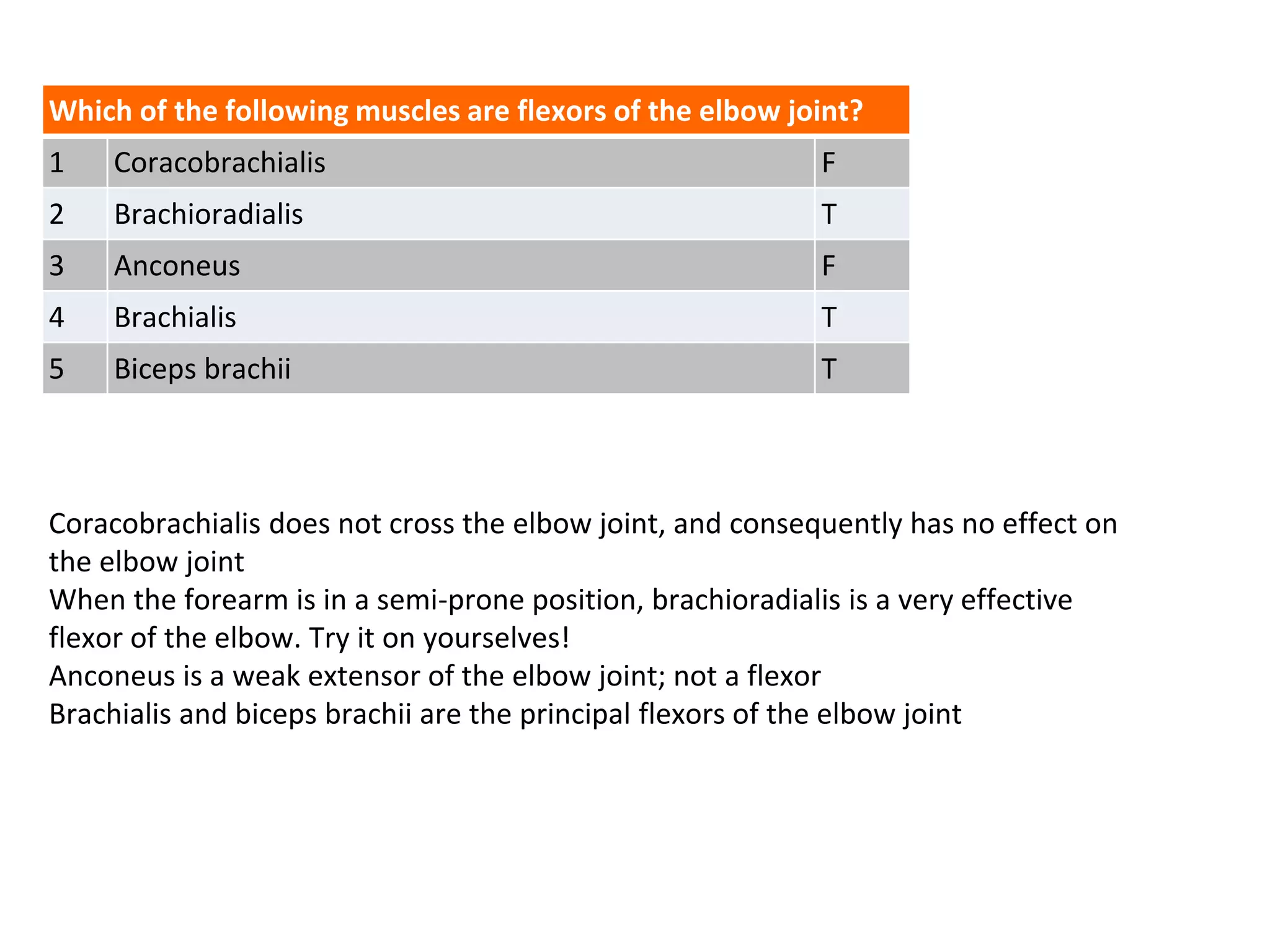

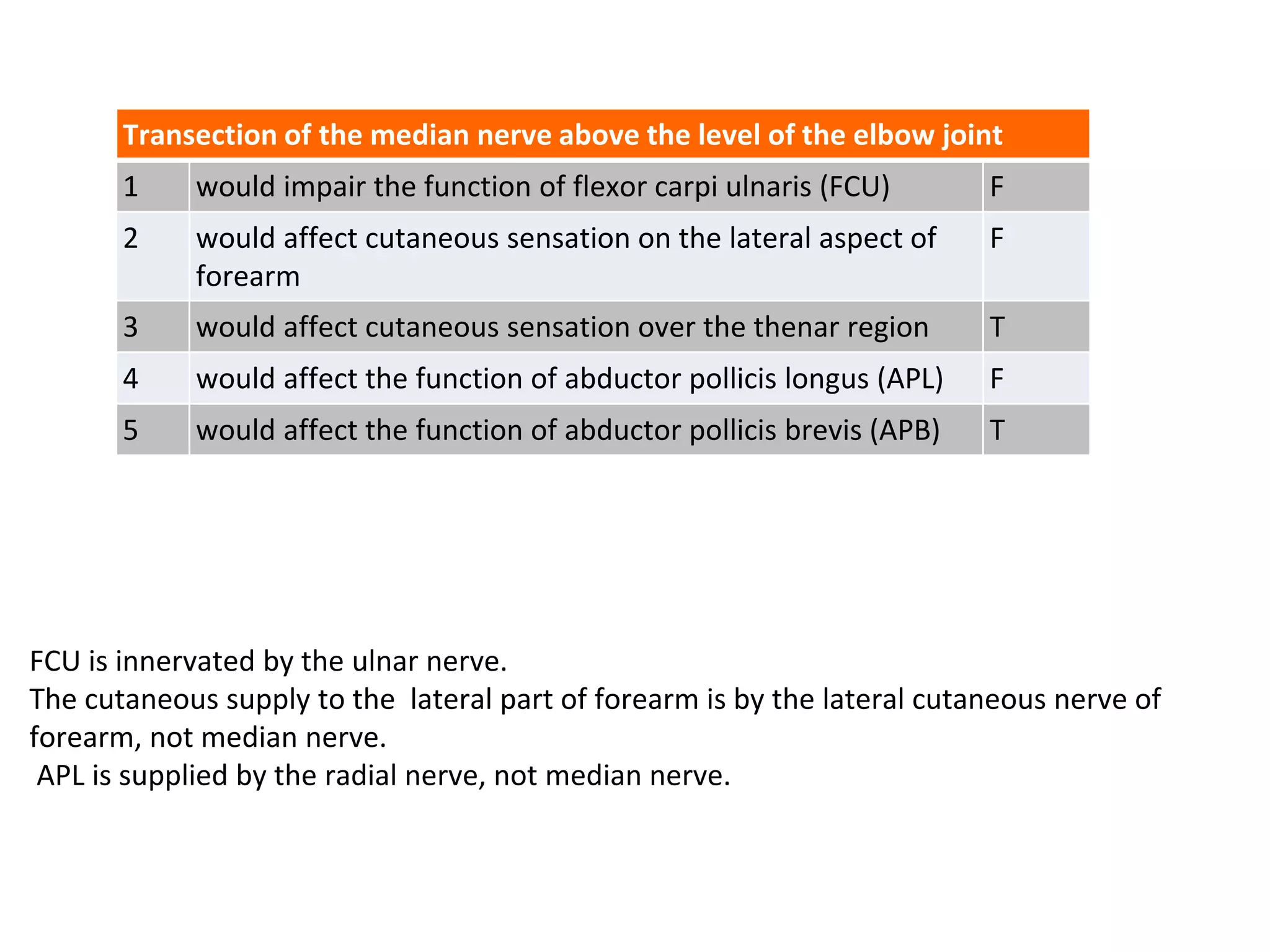


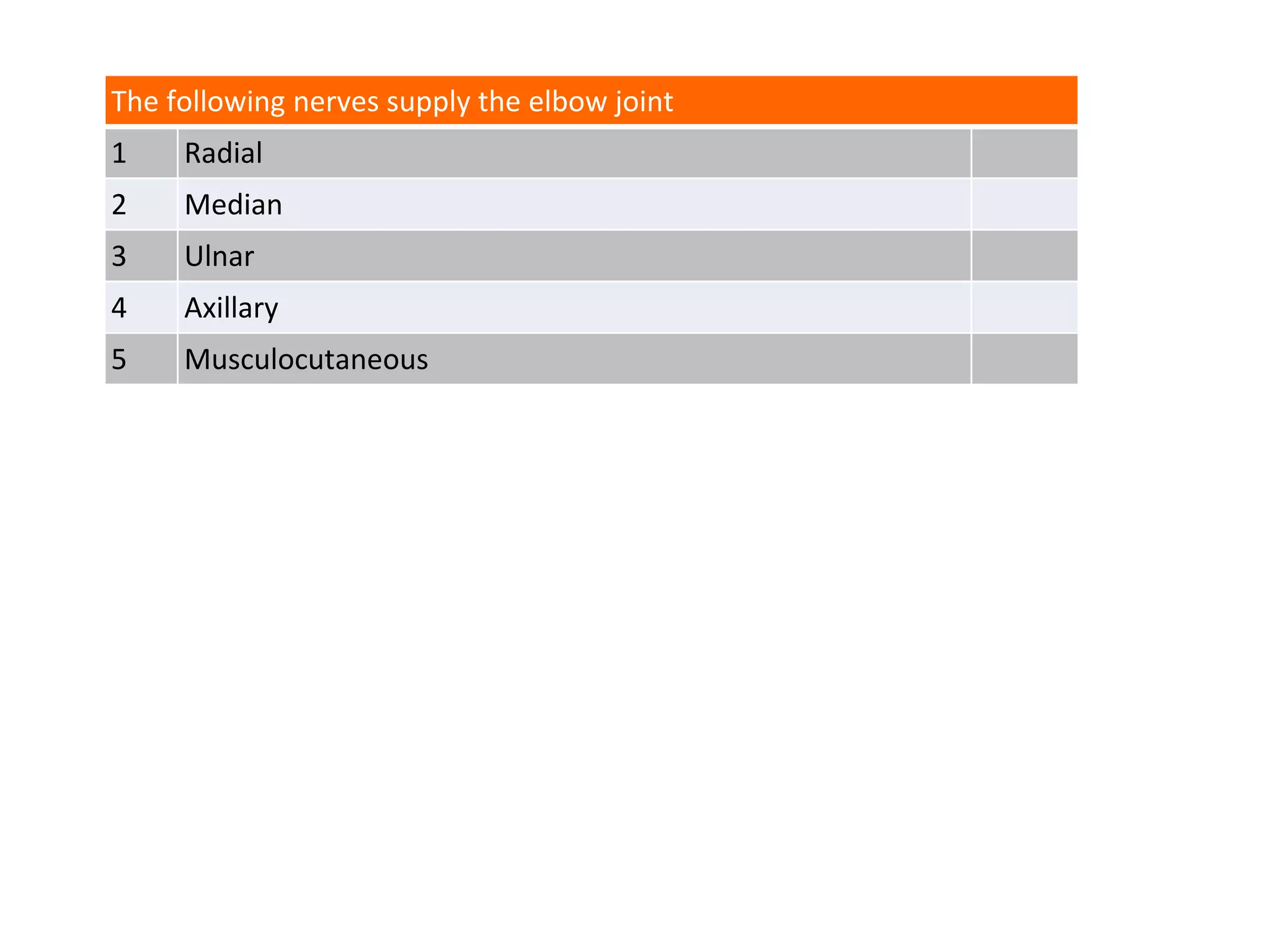
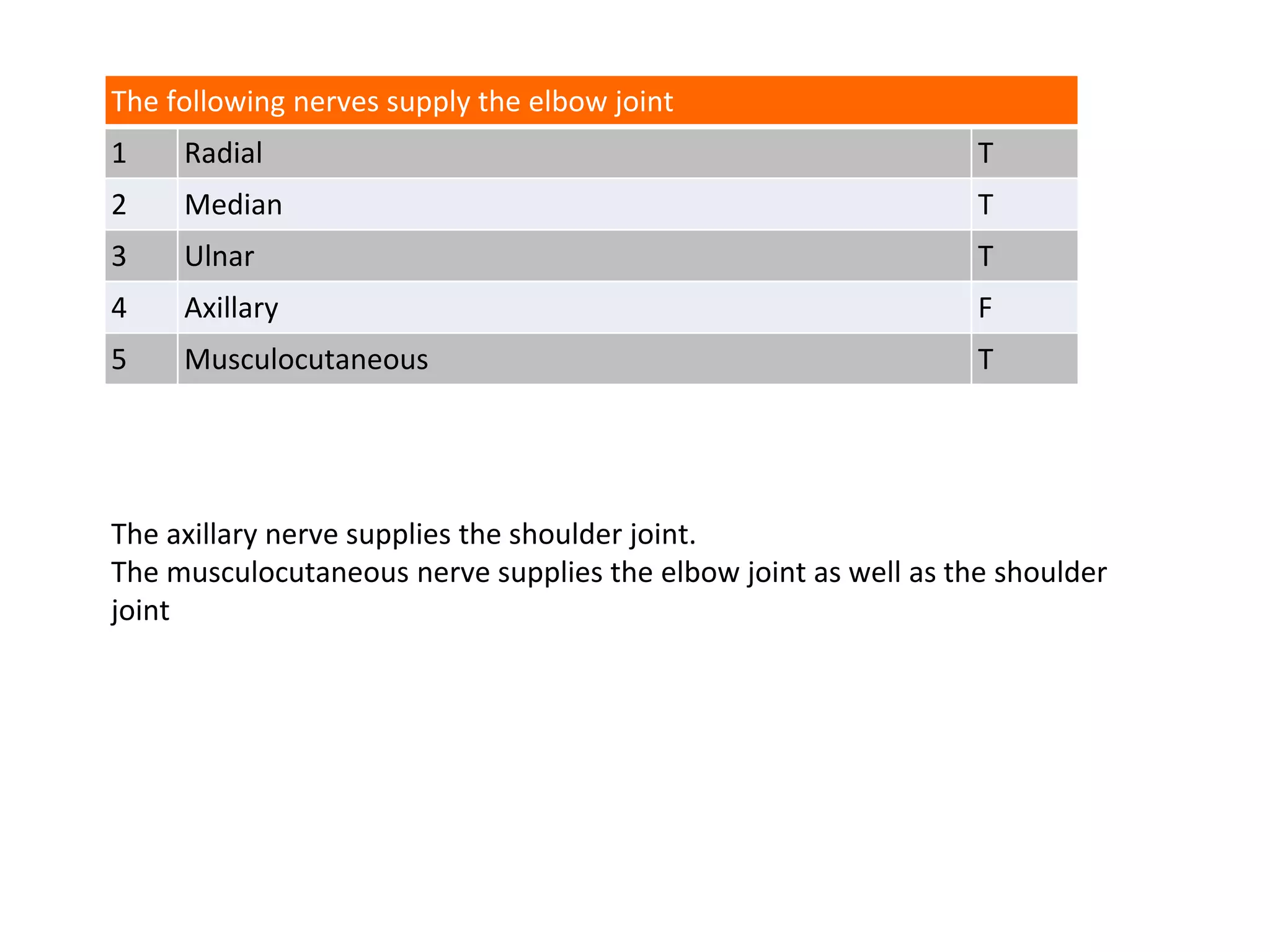

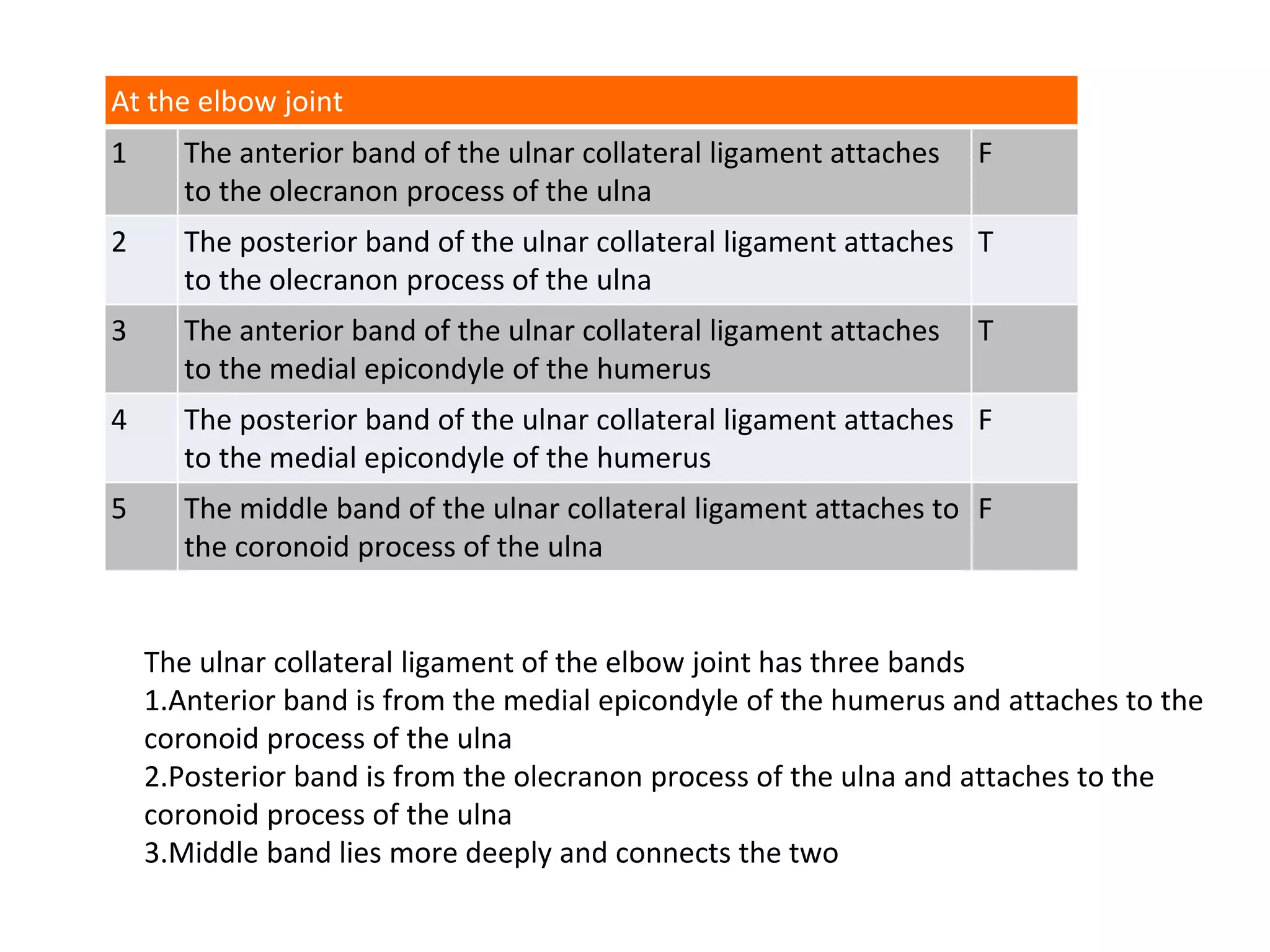



The document discusses the anatomy and function of the elbow joint, including the articulation of the radius and ulna with the humerus and the associated ligaments. It highlights the roles of specific muscles in elbow flexion and the effects of nerve injuries, particularly focusing on the radial and median nerves. Additionally, it details the connections of the ulnar collateral ligament and the structure of various nerves supplying the elbow joint.