• The elbowis the joint connecting the upper arm to the forearm. It is
classed as a hinge-type synovial joint.
• It is a Synovial joint
• Hinge type(Allowing movement only in one plane)
• Compound joint (as there are two articulations in the joint)
3.
Elbow joint isformed by three joints:
•Humeroulnar(Ulnotrochlear) joint
•Humeroradial(Radiocapitellar) joint
•Proximal Radio-Ulnar joint
4.
Structures of theElbow Joint
Articulating Surfaces
• The elbow joint consists of two separate
articulations:
• Trochlear notch of the ulna and the
trochlea of the humerus
• Head of the radius and the capitulum of
the humerus
5.
Bones Articulations CharacteristicsKey palpation points
Humerus
Ulna Humeroulnar joint
Made up of the trochlear groove on the
humerus and the trochlear notch on the
ulna. In the literature, this joint is
described as a modified hinge joint, with
approximately 5 degrees of internal and
external rotation at the extremes of
flexion and extension.[4]
Humerus
Radius Humeroradial joint
Made up of the capitulum of the
humerus and the head of the radius. Due
to its dual action in joint
flexion/extension and
supination/pronation, it is called a
hinge/pivot joint.
To palpate the head of the radius, place
the patient's forearm in a supinated
position. Locate the distal biceps tendon
in the cubital fossa. Next, move your
finger one thumb width laterally and
distally from the biceps tendon, and you
will feel the radial head. To confirm your
palpation, ask the patient to move from
supination to pronation, and you will feel
the radial head rotating.
Radius
Ulna
Proximal radioulnar
joint
Made up of the head of the radius and
the radial notch of the ulna (lesser
sigmoid cavity). The muscles, bones, and
joint capsule provide static and dynamic
stabilisation of this joint.
To palpate the radial notch of the ulna,
locate the olecranon first. Next, move
your fingers gently towards the medial
epicondyle. You will feel a soft, round,
tubular structure, which is the ulnar
nerve on the notch. Firm palpation of this
area compresses the ulnar nerve and can
produce an unpleasant pinprick sensation
which runs down the patient's forearm.
6.
Joint Capsule andBursae
• Like all synovial joints, the elbow joint has a capsule enclosing the
joint. This is strong and fibrous, strengthening the joint. The joint
capsule is thickened medially and laterally to form collateral
ligaments, which stabilise the flexing and extending motion of the
arm.
• A bursa is a sac-like structure containing a small amount of synovial
fluid. It functions to decrease friction between tendons, bone, and
skin during movement. There are many bursae in the elbow, but only
a few have clinical importance:
7.
• Intratendinous olecranon– located within the tendon of the triceps
brachii.
• Subtendinous olecranon – between the olecranon and the tendon of
the triceps brachii, reducing friction between the two structures
during extension and flexion of the arm.
• Subcutaneous olecranon bursa – between the olecranon and the
overlying connective tissue (implicated in olecranon bursitis).
8.
Ligaments
• The jointcapsule of the elbow is strengthened by ligaments medially
and laterally.
• The radial collateral ligament is found on the lateral side of the joint,
extending from the lateral epicondyle, and blending with the annular
ligament of the radius (a ligament from the proximal radioulnar joint).
• The ulnar collateral ligament originates from the medial epicondyle,
and attaches to the coronoid process and olecranon of the ulna.
10.
Blood Supply
• Theelbow joint receives a rich arterial supply from a surrounding
network of vessels, which is formed by branches of the brachial
artery.
Innervation
• The elbow joint is innervated by branches of the medial,
musculocutaneous, radial and ulnar nerves.
11.
Movements
• The orientationof the bones forming the elbow joint produces a
hinge type synovial joint, which allows for extension and flexion of the
forearm:
• Extension – triceps brachii and anconeus
• Flexion – brachialis, biceps brachii, brachioradialis
12.
Injuries to theElbow Joint
• Bursitis
• Subcutaneous bursitis: Repeated friction and pressure on the bursa
can cause it to become inflamed. Because this bursa lies relatively
superficially, it can also become infected (e.g. skin laceration from a
fall on the elbow)
• Subtendinous bursitis: This is caused by repeated flexion and
extension of the forearm, commonly seen in assembly line workers.
Usually flexion is more painful as more pressure is put on the bursa.
13.
Dislocation
• An elbowdislocation usually occurs when a young child falls on a
hand with the elbow flexed. The distal end of the humerus is driven
through the weakest part of the joint capsule, which is the anterior
side. The ulnar collateral ligament is usually torn and there can also be
ulnar nerve involvement
• Most elbow dislocations are posterior, and it is important to note that
elbow dislocations are named by the position of the ulna and radius,
not the humerus.
15.
Epicondylitis (Tennis elbowor Golfer’s elbow)
• Most of the flexor and extensor muscles in the forearm have a common
tendinous origin. The flexor muscles originate from the medial
epicondyle, and the extensor muscles from the lateral. Sportspersons can
develop an overuse strain of the common tendon – which results in pain
and inflammation around the area of the affected epicondyle.
• Typically, tennis players experience pain in the lateral epicondyle from the
common extensor origin. Golfers experience pain in the medial epicondyle
from the common flexor origin. This is easily remembered as golfers aim
for the ‘middle’ of the fairway, while tennis players aim for the ‘lateral’ line
of the court!
16.
Supracondylar Fracture
• Asupracondylar fracture usually occurs due to a fall onto on
outstretched, extended hand in a child (95%) but more rarely can
occur by a direct impact onto a flexed elbow. It is typically
a transverse fracture, spanning between the two epicondyles in the
relatively weak epicondylar region formed by the olecranon fossa and
coronoid fossa which lie opposite each other in the distal humerus.
17.
• Direct damage,or swelling can cause the interference to the blood
supply of the forearm via the brachial artery. The
resulting ischaemia can cause Volkmann’s ischaemic contracture –
uncontrolled flexion of the hand, as flexors muscles become fibrotic
and short. There also can be damage to the medial, ulnar or
radial nerves. As a result, the neurovascular examination and
documentation of all patients presenting with these injuries is vital.
Sometimes, the blood supply can be interrupted acutely leading to a
‘pale, pulseless’ limb often in a child, usually requiring emergency
surgery.
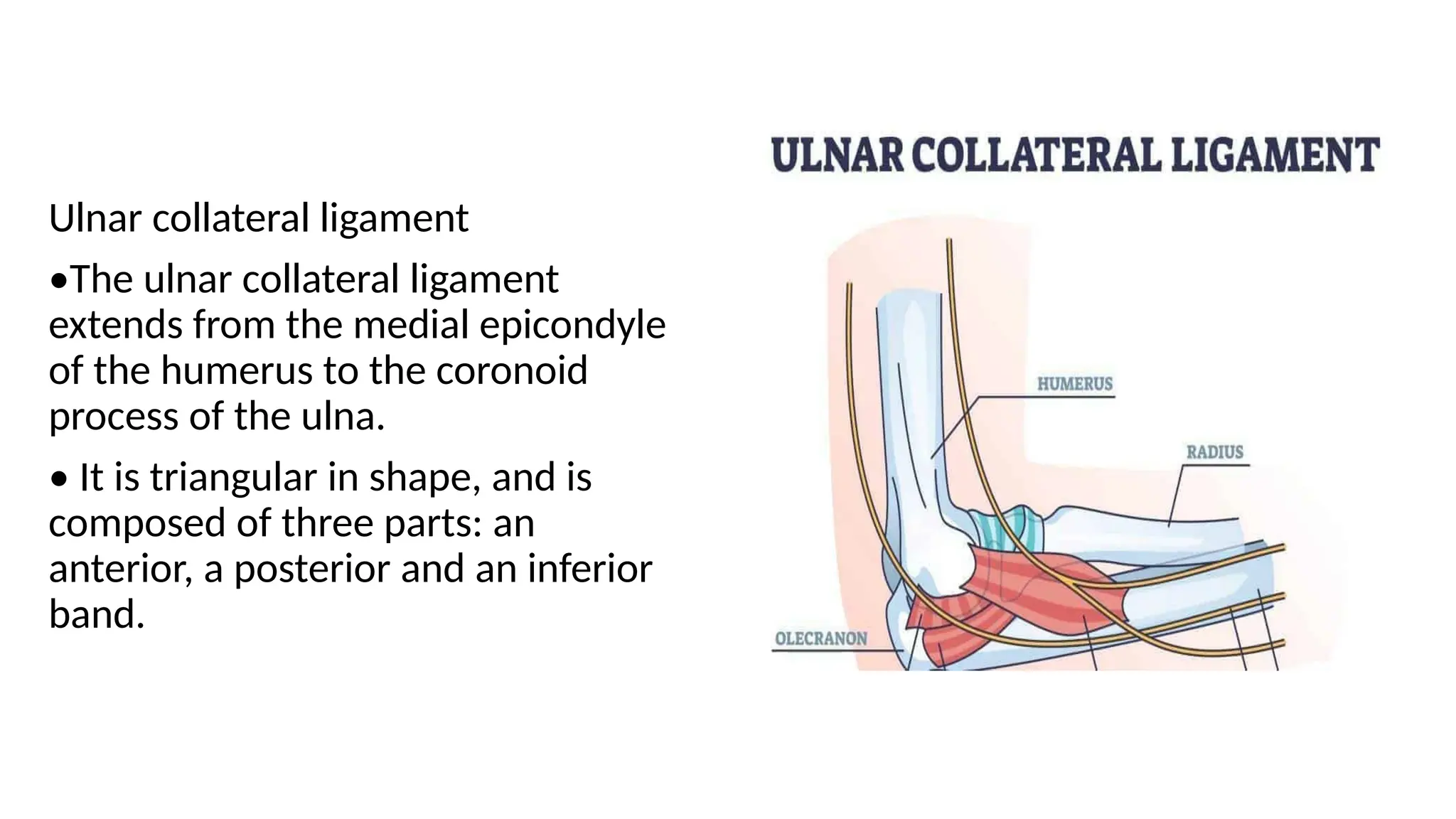
Ulnar collateral ligament
•Theulnar collateral ligament
extends from the medial epicondyle
of the humerus to the coronoid
process of the ulna.
• It is triangular in shape, and is
composed of three parts: an
anterior, a posterior and an inferior
band.
20.
The radial collateralligament
• The radial collateral ligament has a low
attachment to the lateral epicondyle of the
humerus.
• The distal fibers blend with the annular
ligament that encloses the head of the
radius, as well as with the fibers of the
supinator and the extensor carpi radialis
brevis muscles
21.
• The annularligament also
reinforces the joint by holding
the radius and ulna together at
their proximal articulation.
• The quadrate ligament is also
present at this joint, and
maintains constant tension
during pronation and supination
movements of the forearm
22.
Muscles
• Biceps brachiioriginates as two heads
The tendon of the long head originates from the supraglenoid tubercle of the
scapula . It passess through the joint capsule of the shoulder joint and through
the bicipital groove on the anterior surface of the humerus .
The short head of the biceps brachii muscle originates from the coracoid
process of the scapula .these heads join together to form the biceps brachii
muscle belly .
The muscle inserts via a single tendon onto the radial tuberosity distal to the
elbow joint . In the forearm there is a continuation of this tendon as a flattened
connective tissue sheath , the bicipital aponeurosis .
This aponeurosis blends with the deep fascia in the anterior forearm .
23.
• Brachialis originatesfrom the distal half of the anterior surface of the
humerus , as well as from the intermuscular septa on either side of
the anterior compartment
• It is located deep to the biceps brachii muscle. It forms a singular
tendon that inserts onto the tuberosity of the ulna .
24.
• Both thetriceps brachii and brachialis muscles are innervated by the
musculocutaneous nerve .
• While the biceps brachii and the brachialis muscles are the main
flexors of the elbow joint ,the brachioradialis muscle is also involved in
the flexion of the forearm at this joint.
• Brachioradialis originated from the lateral aspect of the distal
humerus above the lateral epicondyle .
• It inserts onto the lateral aspect of the distal radius . Although this
mucle is primarily in the forearm, it crosses the elbow joint so
therefore it acts on the elbow joint.it is innervated by the radial nerve
25.
• Triceps brachiioriginates from the infra glenoid tubercle of the
scapula , the lateral head originates from the lateral aspect of the
humerus above the radial groove , and the medial head orginates
from the media; aspect of the humerus below the level of the radial
groove .
• The three heads converge on a single tendon that inserts onto the
olecranon of the ulna . It is supplied by the radial nerve , which passes
down through the arm in the radial groove between the lateral and
medial heads of the muscle .
26.
• While flexionand extension are the only movements that can occur the
at the elbow joint itself , movements is also afforded at the proximal
radioulnar joint , which contributes to the elbow joint.
• Movements at this joint are called pronation and supination the distal
• These are rotational movements that occur when the distal end of the
radius moves over the distal end of the ulna by rotating the radius in
the pivot joint formed by the circular head of the radius , the radial
groove of the ulna and the annular ligament .




![Bones Articulations Characteristics Key palpation points
Humerus
Ulna Humeroulnar joint
Made up of the trochlear groove on the
humerus and the trochlear notch on the
ulna. In the literature, this joint is
described as a modified hinge joint, with
approximately 5 degrees of internal and
external rotation at the extremes of
flexion and extension.[4]
Humerus
Radius Humeroradial joint
Made up of the capitulum of the
humerus and the head of the radius. Due
to its dual action in joint
flexion/extension and
supination/pronation, it is called a
hinge/pivot joint.
To palpate the head of the radius, place
the patient's forearm in a supinated
position. Locate the distal biceps tendon
in the cubital fossa. Next, move your
finger one thumb width laterally and
distally from the biceps tendon, and you
will feel the radial head. To confirm your
palpation, ask the patient to move from
supination to pronation, and you will feel
the radial head rotating.
Radius
Ulna
Proximal radioulnar
joint
Made up of the head of the radius and
the radial notch of the ulna (lesser
sigmoid cavity). The muscles, bones, and
joint capsule provide static and dynamic
stabilisation of this joint.
To palpate the radial notch of the ulna,
locate the olecranon first. Next, move
your fingers gently towards the medial
epicondyle. You will feel a soft, round,
tubular structure, which is the ulnar
nerve on the notch. Firm palpation of this
area compresses the ulnar nerve and can
produce an unpleasant pinprick sensation
which runs down the patient's forearm.](https://image.slidesharecdn.com/elbow-251204035756-26e3bf65/75/elbow-SRUCTURES-MUSCLES-CUBITAL-FOSSA-ATTACHMENTS-5-2048.jpg)