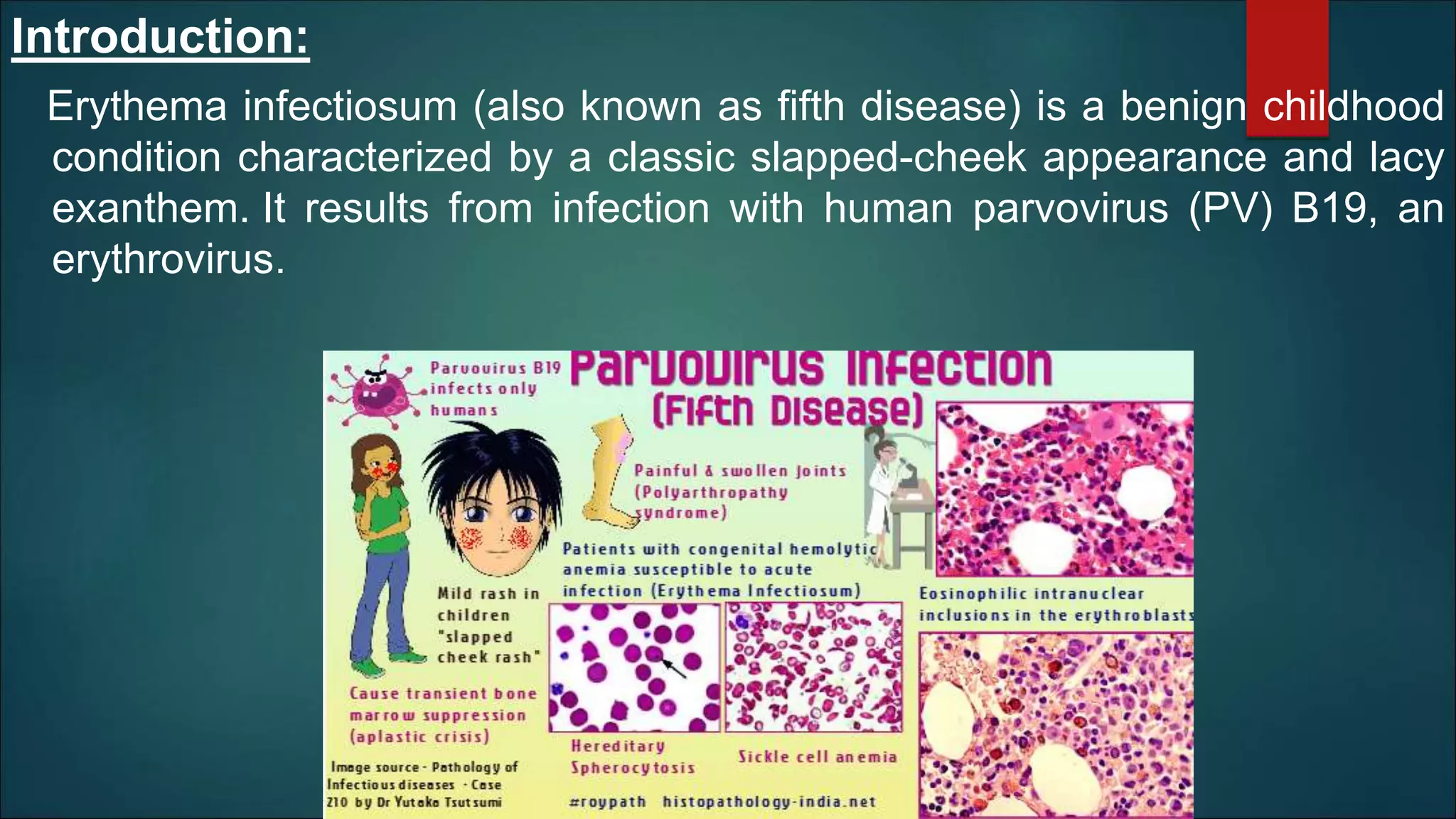
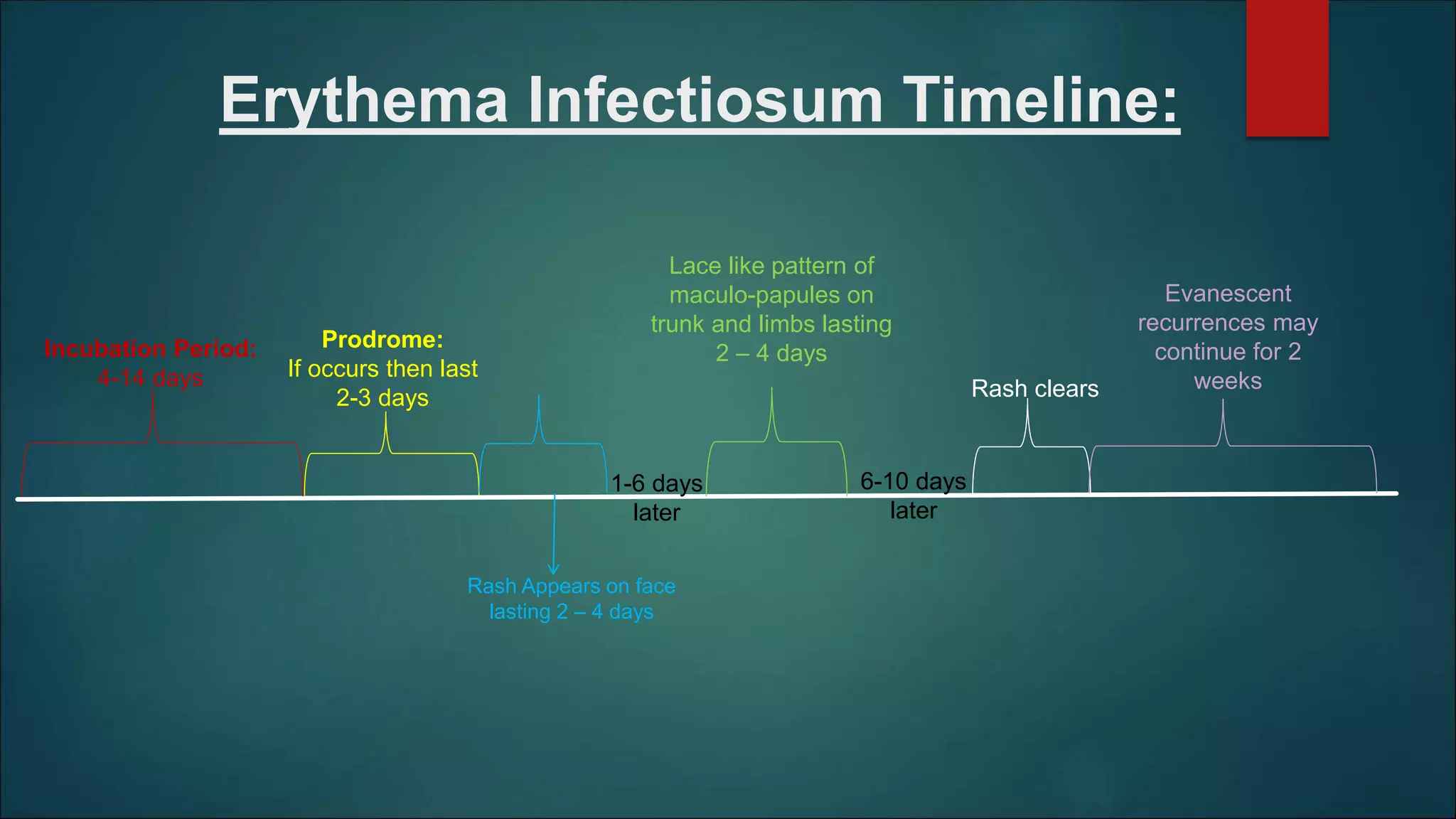
Erythema infectiosum, or fifth disease, is a benign childhood illness caused by human parvovirus B19 that presents with a slapped-cheek appearance and lacy rash. It primarily spreads through respiratory droplets and can affect adults, often leading to polyarthralgia. The condition is self-limiting, with a typical duration of 6-10 days, and no specific treatment is required, although pregnant women and the immunocompromised may need careful monitoring.