Download as PDF, PPTX


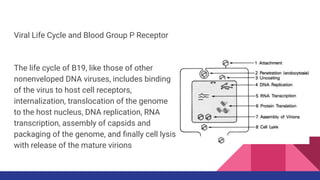



1. Parvovirus B19 causes a range of clinical manifestations from asymptomatic infection to transient erythroblastopenia or aplastic crisis depending on the host's immune status and underlying medical conditions. 2. The virus binds to the P blood group antigen receptor on erythroid progenitor cells and causes their lysis, resulting in transient red cell aplasia. This causes a temporary anemia in healthy individuals but can cause a severe aplastic crisis in those with hemolytic anemia. 3. Diagnosis involves detecting B19 viral DNA by PCR or antibodies such as IgM, which indicates a current infection, and IgG which persists for life after infection and confers immunity.







































































![Polymer [ बहुलक ] Chemistry Notes PDF - Irfanullah Mehar - JJ Sir Chemistry.pdf](https://cdn.slidesharecdn.com/ss_thumbnails/polymerchemistrynotespdf-irfanullahmehar-jjsirchemistry-260210172118-3f9b37f7-thumbnail.jpg?width=640&height=640&fit=bounds)














