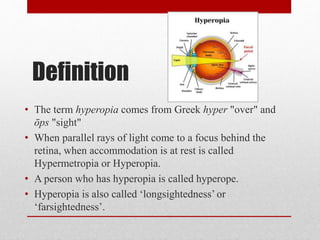
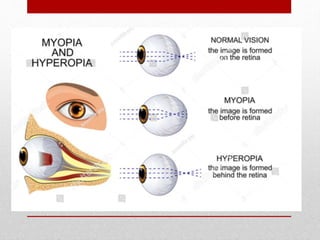
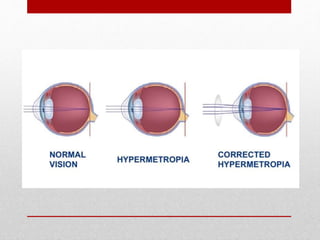
Hypermetropia, or hyperopia, is a refractive error where light focuses behind the retina, causing difficulty in near vision and potentially leading to symptoms such as eyestrain and headaches. It can be classified by anatomical features, degree, and its effects on accommodation, with specific types including axial, curvature, and index hypermetropia. Treatment options include optical methods like glasses and contact lenses, as well as surgical procedures.