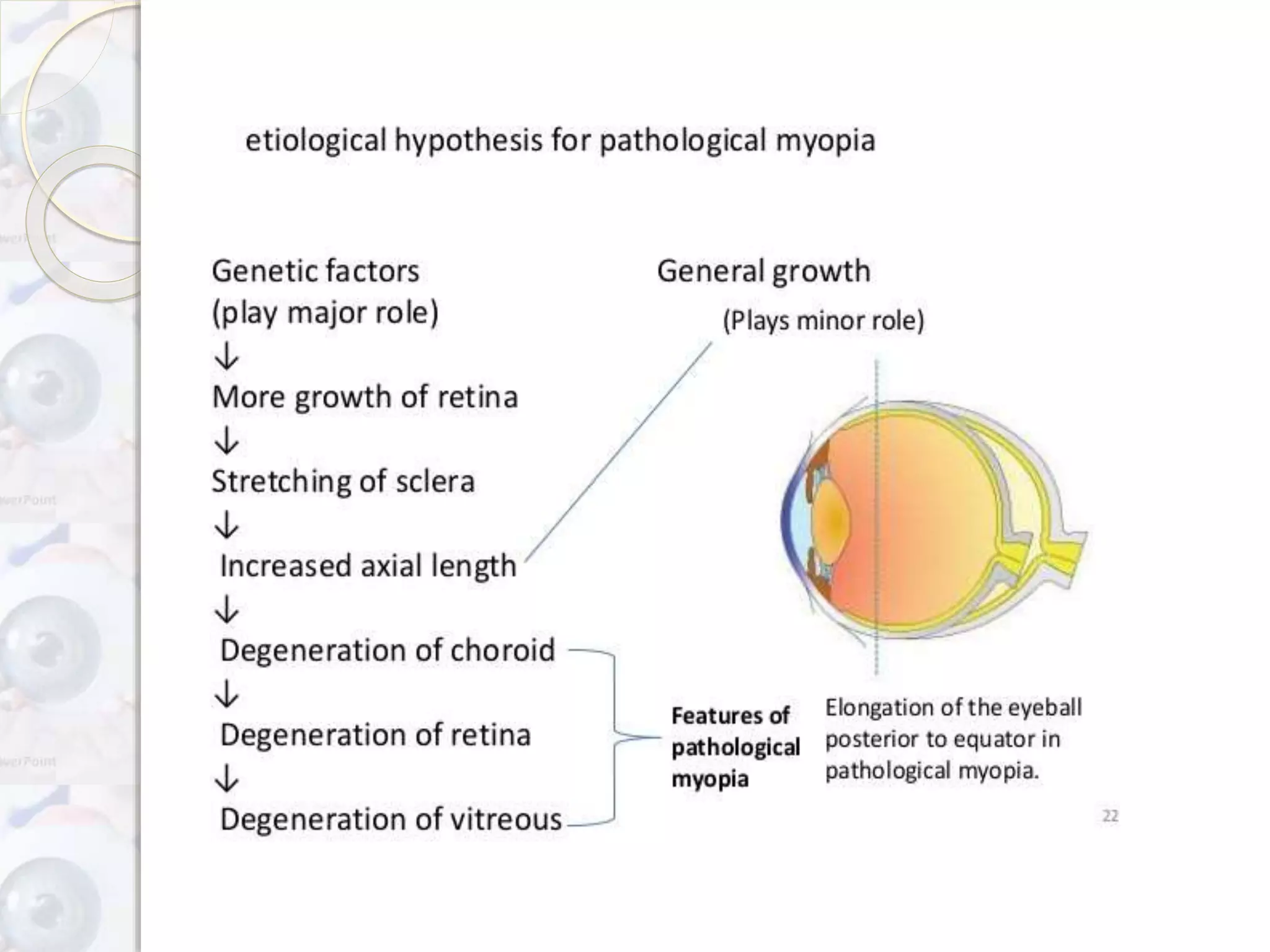
The document discusses myopia, a refractive error characterized by difficulty in seeing distant objects. It categorizes myopia into various types such as congenital, simple, pathological, and acquired, outlining their causes, symptoms, and management strategies. Treatment options include optical correction with lenses, surgical interventions, and preventive measures to manage the progression of myopia.