This document discusses the anatomy and ventilation patterns of the epitympanum. It describes:
1) The epitympanum is divided into anterior and posterior compartments. The superior attic communicates with the mesotympanum via the isthmus and is ventilated through the isthmus. The inferior lateral attic and Prussak space are ventilated by the mesotympanum.
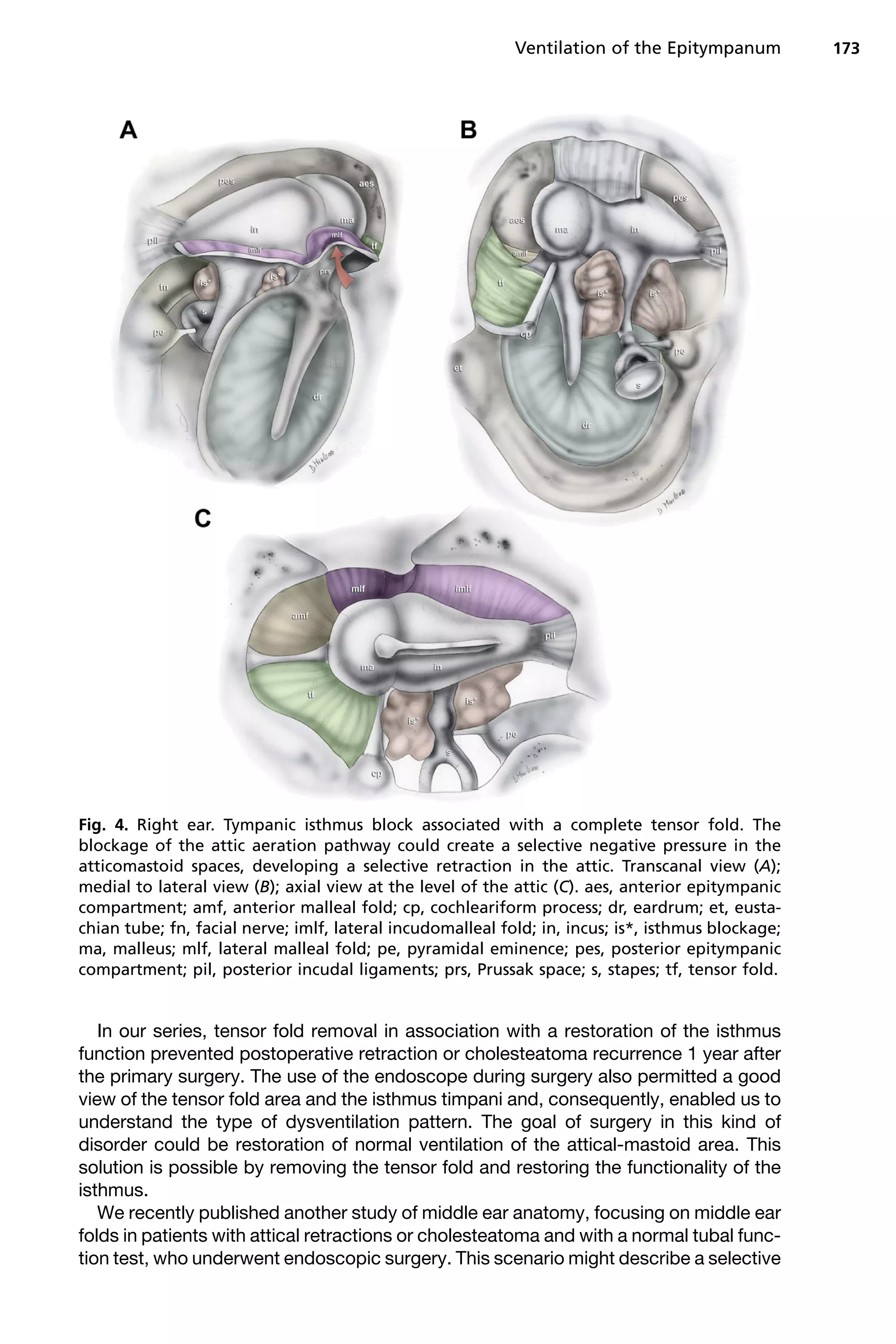
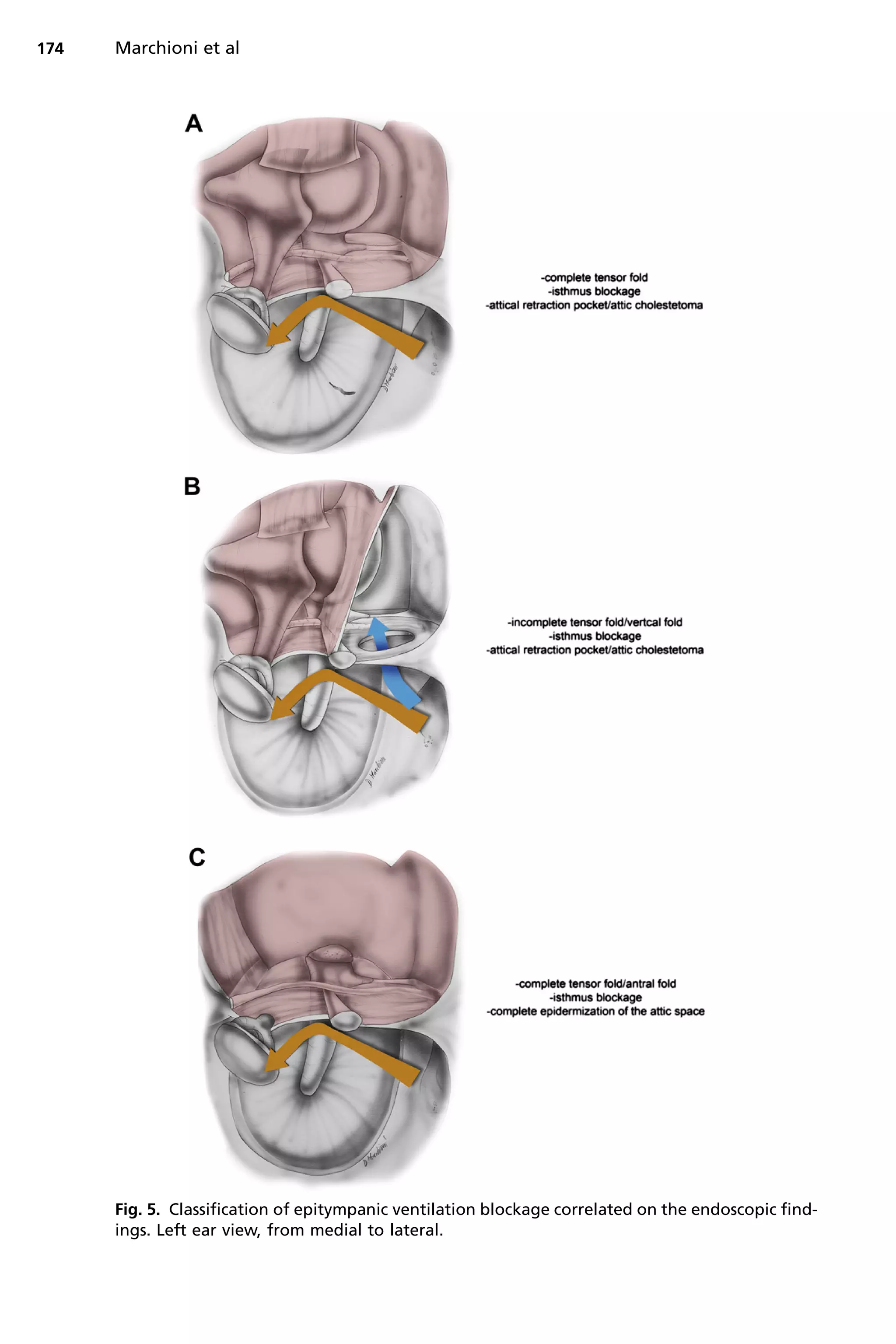
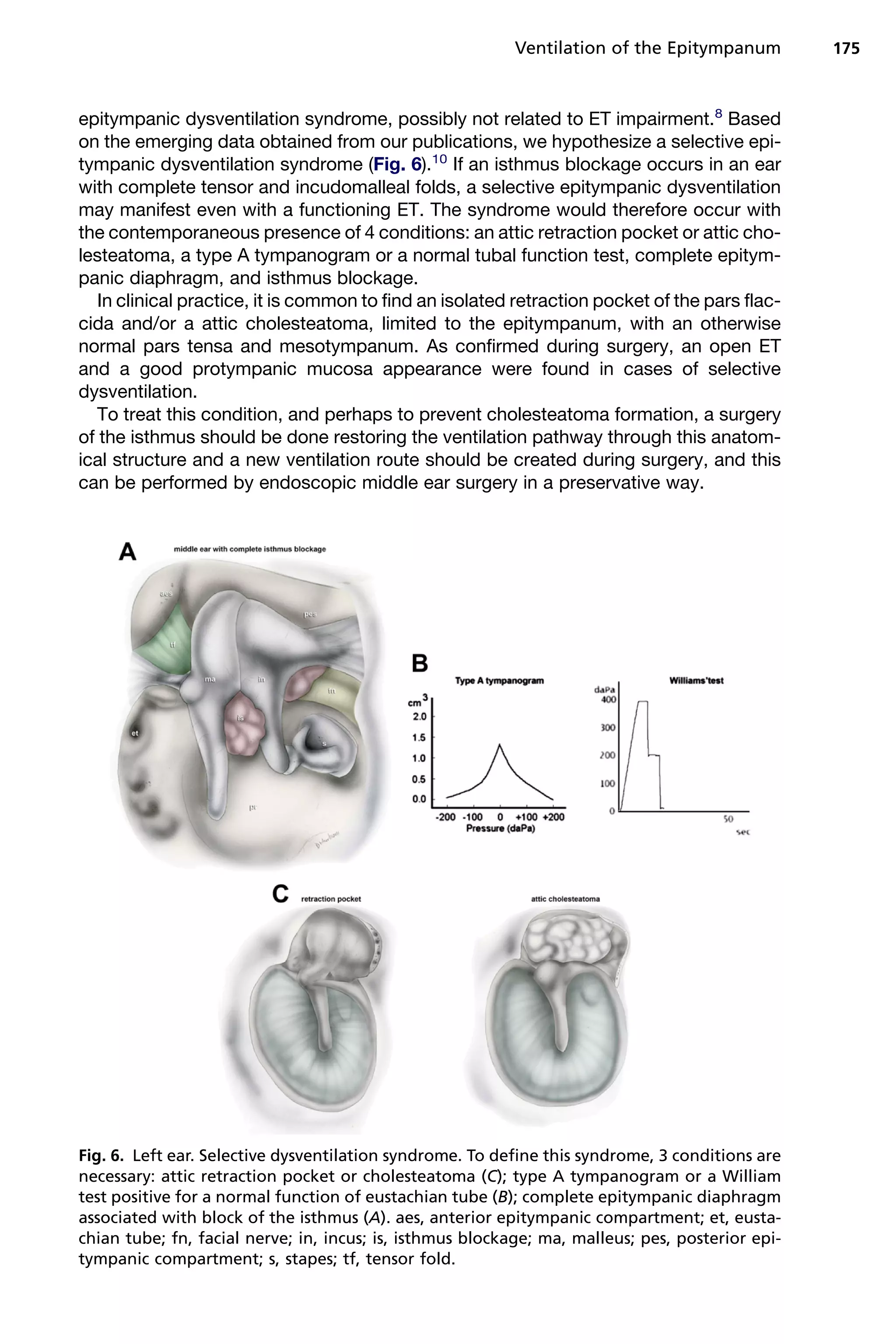
2) The tensor fold plays a role in ventilation, and can be complete or incomplete. A complete tensor fold with isthmus blockage can lead to inadequate ventilation and attic retraction.
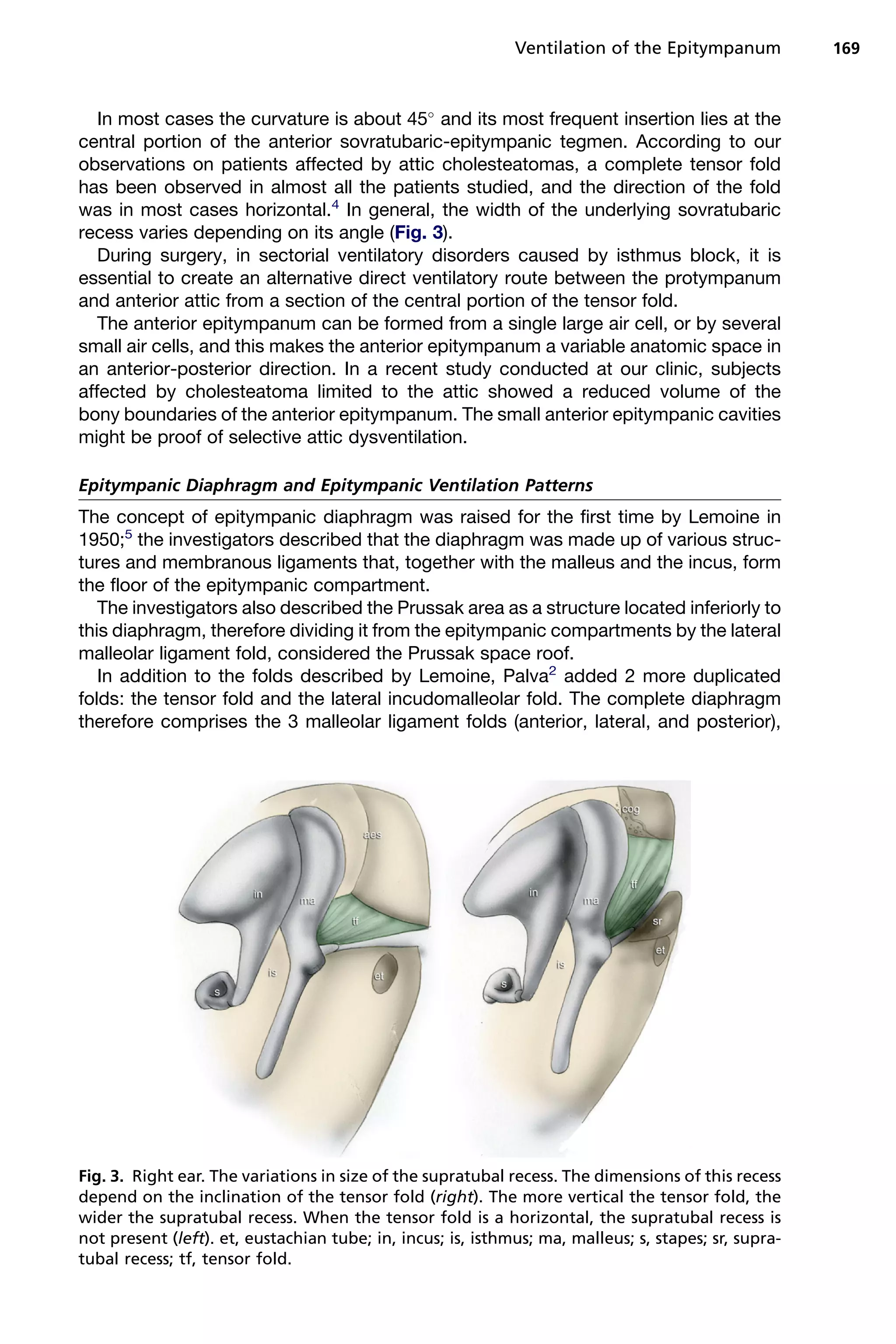
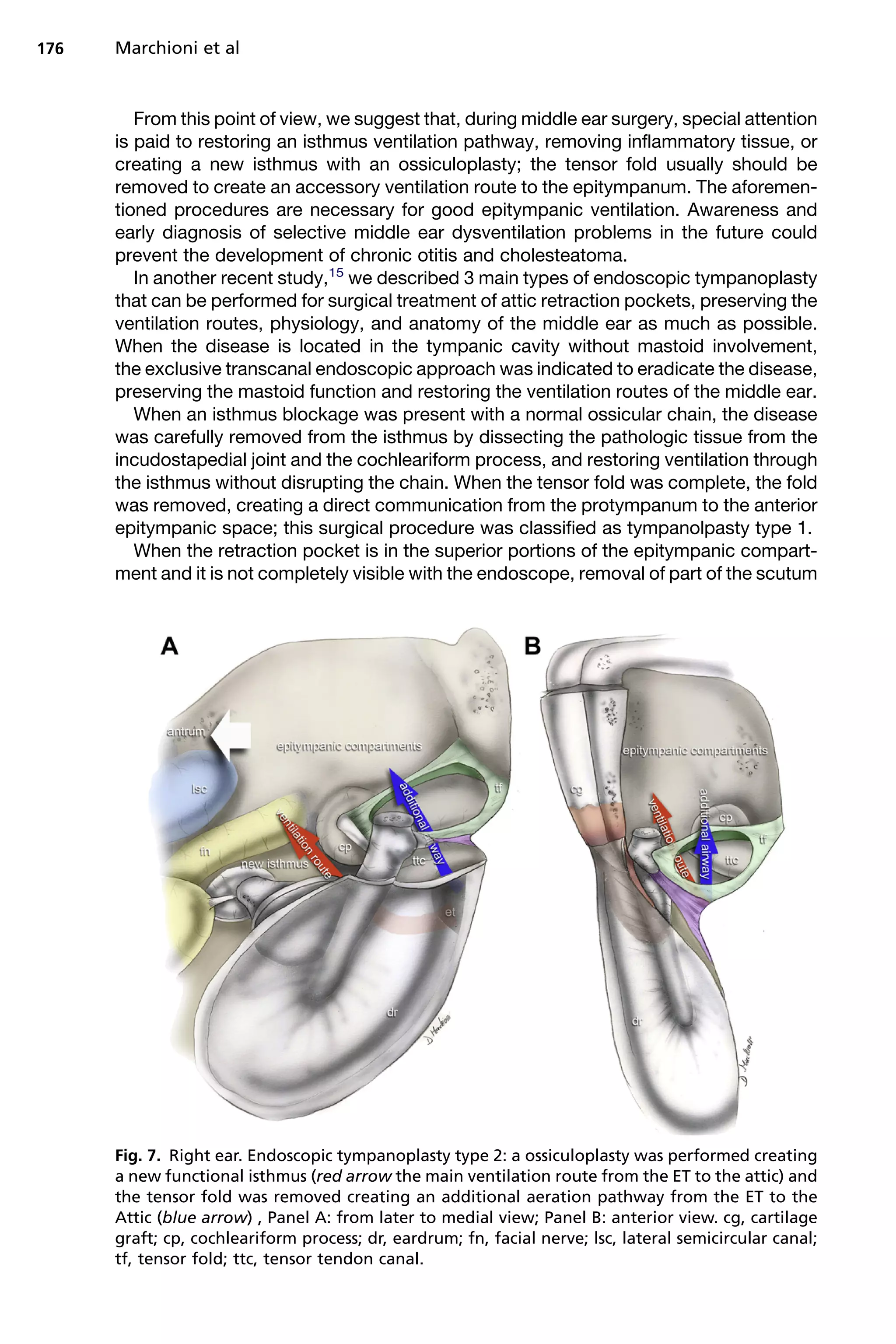
3) Endoscopic surgery aims to restore ventilation by enlarging the isthmus and