
Recommended
More Related Content
What's hot
What's hot (20)
Similar to THE MIDDLE EAR
Similar to THE MIDDLE EAR (20)
More from Suraj Dhara
More from Suraj Dhara (20)
Recently uploaded
Recently uploaded (20)
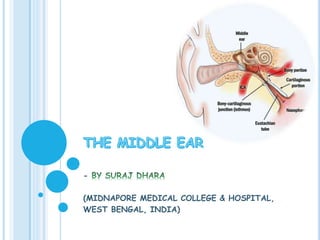
THE MIDDLE EAR
- 1. - (MIDNAPORE MEDICAL COLLEGE & HOSPITAL, WEST BENGAL, INDIA)
- 2. 2
- 3. INTRODUCTION Middle ear cavity is also known as tympanic cavity. Remember Tympanoplasty is an operative approach to the tympanic cavity (eradicate disease from middle ear cavity by ossicular reconstruction & improves hearing) with or without an approach to tympanic membrane (Myringoplasty = Type 1 Tympanoplasty). Middle ear together with Eustachian tube, aditus, antrum and mastoid air cells are called middle ear cleft. It is lined by secretory mucosa & filled with air. 3 drsurajmmch
- 5. PARTS In relation to the tympanic membrane it is divided into Epitympanum / Attic : above the pars tensa but medial to the Shrapnell’s membrane & bony lateral attic wall (scutum). Mesotympanum : lying opposite the pars tensa. Hypotympanum : lying below the level of pars tensa. The portion of middle ear around the tympanic orifice of Eustachian tube is called protympanum. 5 drsurajmmch
- 7. BOX REPRESENTATION Middle ear can be compared with a six walled room with a roof, a floor, medial, lateral, anterior & posterior walls. 7 drsurajmmch
- 8. ROOF Thin plate of bone called tegmen tympani. It extends posteriorly as tegmen antri to form roof of the mastoid antrum. Roof separates tympanic cavity from middle cranial fossa. Tegmen is bulged, called arcuate eminence due to superior semicircular canal. 8 drsurajmmch
- 9. FLOOR Separates from jugular bulb. Sometimes it is congenitally deficient & jugular bulb may then project into middle ear only covered by mucosa. In the floor there is carotico-jugular crest, which can be normally distinguished by CT-scan. Anterior to which internal carotid artery & posterior to which jugular bulb is present. Inability to distinguish JB & ICA in CT-scan due to erosion of the crest called Phelp sign. Seen in contrast enhanced CT-scan of glomus tumor. 9 drsurajmmch
- 11. 11 Just focus on 11 & 12 (ICA & JB) & the crest between them (not shown but imagine) drsurajmmch
- 12. ANTERIOR WALL Two openings are there 12 drsurajmmch
- 13. 13 1 : Canal for tensor tympani muscle 2 : Eustachian tube drsurajmmch
- 14. MEDIAL WALL 14 Oval window / Fenestra vestibuli – to which footplate of the stapes attaches. Round window / Fenestra cochleae – covered by secondary tympanic membrane. Promontory – bulged due to 1st or basal coil of cochlea. Processus cochleariformis – anterior to oval window a hook like projection. Tensor tympani muscle after originating from canal for TT on anterior wall hooks around this projection and attaches to neck of malleus. Supplied by mandibular br. of trigeminal nv (5th). It also marks the level of 1st genu of facial nerve, an important landmark for surgery of facial nv. drsurajmmch
- 15. MEDIAL WALL Facial nerve – above the oval window a bony fallopian canal for facial nv (horizontal / tympanic part). Its bony covering may sometimes be congenitally dehiscent making the nv vulnerable to injury & infections. Dome of lateral semicircular canal – above the nv canal. Most common site of labyrinthine fistula. 15 drsurajmmch
- 16. 1616 3 : Oval window 4 : Round window 5 : Processus cochleariformis 6 : Dome of lateral / horizontal scc 7 : Facial nerve drsurajmmch
- 17. 17 drsurajmmch
- 18. NARROWEST PART OF MIDDLE EAR ?? 18 TM Promontory Mesotympanum drsurajmmch
- 19. SURGICAL FLOOR OF MIDDLE EAR ?? Width of ME = Depth of ME cavity in surgical position. So shallowest part of middle ear is again mesotympanum. 1919 TM Promontory Medial wall drsurajmmch
- 20. POSTERIOR WALL Lies close to mastoid air cells. Pyramid – bony projection Stapedius muscle appears from the summit of it & gets attached to neck of stapes. Supplied by the nerve to stapedius, a branch of the facial nerve. Aditus – through it attic communicates with antrum. Facial nerve – vertical / mastoid segment runs just behind the pyramid. Gives a branch (chorda tympani) which comes out of anterior wall (through canal of Hugier) by crossing the middle ear simulating a hanging cord. 20 drsurajmmch
- 21. 21 8 : Pyramid 9 : Aditus 10 : Chorda tympani nv drsurajmmch
- 22. POSTERIOR WALL Facial recess / Posterior sinus – depression in the post wall lateral to the pyramid. 22 Facial reccess Laterally Annulus Medially Facial nv Inferiorly Chorda-facial angle Superiorly Fossa incudes (short process) drsurajmmch
- 23. UNDERSTAND THE ORIENTATION 23 Facial recess is the site for posterior tympanotomy / approaching middle ear without disturbing posterior meatal wall. drsurajmmch
- 24. Posteriorly Posterior wall SINUS TYMPANI – 3D SPACE Medial to pyramid. Most common site for recurrent cholesteatoma. 24 Sinus tympani Laterally Facial nv Medially Medial wall Superiorly Ponticulus Inferiorly subiculum drsurajmmch
- 26. LATERAL WALL Largely by tympanic membrane. Lesser extent by scutum. Through the semitransparent tympanic membrane this structures are visible Long process of incus Incudostapedial joint Round window 26 drsurajmmch
- 27. Erosion of scutum (arrow) is a characteristic CT scan finding of cholesteatoma. 27 drsurajmmch
- 28. SHORT TEST !!! Identify the structures : 28 drsurajmmch
- 29. 29 1. Promontory 2. Processus cochleariformis 3. Horizontal part of CN VII 4. Oval window 5. Dome of horizontal canal 6. Pyramid 7. Ponticulus 8. Sinus tympani 9. Subiculum 10. Round window 11. Tympanic plexus drsurajmmch
- 30. OSSICLES The ossicles conduct sound energy from the tympanic membrane to the oval window. There are three middle ear ossicles. Malleus (Hammer) : It consists of a head, neck, handle (manubrium), a lateral and an anterior process. It is the largest ossicle and measures 8 mm in length. Head and Neck: They lie in the attic. Manubrium (handle): It is embedded in the fibrous layer of the tympanic membrane. Anterior process: bony spicule connected to petrotympanic fissure by ligamentous fibres. Lateral process: It appears as a knob-like projection on the outer surface of the tympanic membrane and provides attachments to the anterior and posterior malleal folds. 30 drsurajmmch
- 31. Incus (Anvil) : It consists of following parts: Body and Short process: They lie in the attic. Short pr. is connected to fossa incudis by lig. fibres in epitympanic recess. Long process: It hangs vertically and medial & parallel to malleus handle and forms incudostapedial joint with the head of stapes by its lenticular process. Stapes (Stirrup) : This smallest bone of body measures about 3.5 mm. It consists of head, neck, anterior and posterior crura and footplate. The footplate is positioned in the oval window by annular ligament 31 drsurajmmch
- 32. 32 drsurajmmch
- 33. ARTICULATIONS OF THE OSSICLES 33 drsurajmmch
- 34. LIGAMENTS Malleus Anterior ligament of Malleus: neck of malleus to ant wall of tympanic cavity. Contains muscle fibers called as Laxator tympani/ Musculus externus mallei. Lateral ligament of Malleus: triangular band, from post border of tympanic inscisure to head of malleus. Superior ligament of Malleus: head of malleus to roof of epitympanic recess. Incus Posterior ligament of Incus: from end of short process to fossa incudes. Superior ligament of Incus: body to roof of epitympanic recess. Stapes Vestibular surf & rim of stapedial base covered with hyaline cartilage, which is attached to margin of fenestra vestibuli by annular ligament. 33 drsurajmmch 34
- 35. MUSCLES Tensor tympani: It runs above the eustachian tube in a bony tunnel. Its tendon turns round the processus cochleariformis and passes laterally. Origin: from the bony tunnel, the cart. part of Eustachian Tube & the adjoining part of greater wing of Sphenoid. Insertion: Just below the neck of malleus. N/S: It develops from the 1st branchial arch and is supplied by a branch of the nerve to medial pterygoid, a br of mandibular division of trigeminal nerve (CN V3). B/S: sup. tympanic br of middle meningeal artery Action : It tenses the tympanic membrane by drawing the handle of malleus medially. 35 drsurajmmch
- 36. Stapedius : On contraction it dampens the loud sounds and prevents noise trauma to the inner ear. Origin: Conical cavity and canal within pyramid (on post. tymp wall). Insertion: It inserts to the neck stapes. N/S: It is developed from the 2nd branchial arch and is supplied by a branch of CN VII (nerve to stapedius of facial nerve) B/S: branches of Posterior auricular, anterior tympanic & middle meningeal arteries Action: damp down excessive sound vibrations. Opposes action of tensor tympani which pushes the stapes more tightly into fenestra vestibuli. 36 drsurajmmch
- 37. 37 drsurajmmch
- 38. INTRATYMPANIC NERVES Tympanic plexus (Nerve supply of middle ear) : The tympanic nerve plexus, which lies on the promontory, supplies to the medial surface of the tympanic membrane, tympanic cavity, mastoid air cells and the bony eustachian tube. It is formed by following nerves: Tympanic branch of glossopharyngeal (Jacobson’s Nerve) : It carries secretomotor fibers to the parotid gland. The pathway of secretomotor fibers to the parotid gland consists of Inferior salivary nucleus - CN IX - Jacobson’s tympanic branch - Tympanic plexus - Lesser petrosal nerve - Otic ganglion - Auriculotemporal nerve - Parotid gland. Section of Jacobson’s nerve is carried out in cases of Frey’s syndrome. Sympathetic fibers : Caroticotympanic nerves come from the sympathetic plexus, which is present round the internal carotid artery 38 drsurajmmch
- 39. Chorda tympani nerve: This branch of the facial nerve enters the middle ear through posterior canaliculus. It runs on the medial surface of the tympanic membrane. It lies between the malleus and long process of incus, above the insertion of tensor tympani. It carries gustatory fibers from the anterior two- third of tongue and parasympathetic secretomotor fibers to the submaxillary and sublingual salivary glands. 39 drsurajmmch
- 40. 40 drsurajmmch
- 41. FUNCTIONS OF ME Conduction of sound from tympanic membrane to labyrinth. Impedance matching mechanism : when sound travels from ME to IE, maximum wave is reflected back due to impedance of labyrinthine fluid. So ME does this actions Lever action of ossicles : handle of malleus is 1.3 times longer than long process of incus, providing mechanical advantage of 1.3 Hydraulic action of tympanic membrane : Total area of TM – 90 sq mm. Effective vibratory area of TM – 55 sq mm. Area of footplate of stapes – 3.2 sq mm. Areal ratio – 17 : 1 Total transformer ratio - 17 x 1.3 = 22 : 1 41 drsurajmmch
- 42. 42 Total area of TM – 90 sq mm. Effective vibratory area of TM – 55 sq mm. Area of footplate of stapes – 3.2 sq mm. Areal ratio – 17 : 1 drsurajmmch
- 43. MASTOID ANTRUM This air-containing space (9 mm height, 14 mm width and 7 mm depth) is situated in the upper part of mastoid. Vol – 1ml BOUNDARIES - Roof: It is formed by the tegmen antri, which separates mastoid antrum from the middle cranial fossa. Lateral wall: It is formed by a 15mm thick plate of squamous part of temporal bone which is marked on the lateral surface of mastoid by suprameatal (MacEwen’s) triangle. It is covered by postaural skin. 43 drsurajmmch
- 44. Medial wall: It is formed by the petrous bone and related to the Posterior semicircular canal Endolymphatic sac Dura of posterior cranial fossa. Anterior: Anteriorly mastoid antrum communicates with the attic through the aditus ad antrum. Medial to lateral relations are following: Facial nerve canal Aditus ad antrum and facial recess lie between tympanum and mastoid antrum Deep bony external auditory canal (EAC) 44 drsurajmmch
- 45. Posterior wall: It is formed by mastoid bone and communicates with mastoid air cells. Sigmoid sinus curves downwards. Floor: It is formed by mastoid bone and communicates with mastoid air cells. Other deeper relations from medial to lateral sides are Jugular bulb medial to facial canal. Digastric ridge which gives origin of posterior belly of digastric muscle. Origin of sternocleidomastoid muscle. 45 drsurajmmch
- 46. MACEWEN’S TRIANGLE Linea temporalis (temporal line): A ridge of bone extending posteriorly from the zygomatic process (marking the lower margin of temporalis muscle and approximating the floor of middle cranial fossa) EAC: Posterosuperior margin of EAC. Tangent: A tangent to the posterior margin of EAC . At birth its 2mm thick and increases at rate of 1 mm/yr to attain full thickness of 12-15mm. 46 drsurajmmch
- 47. 47 drsurajmmch
- 48. 48 drsurajmmch
- 49. MASTOID The mastoid consists of bony cortex with a honeycomb of air cells underneath. Depending on development of air cells, three types of mastoid have been described. Well pneumatized / Cellular – well developed air cells with thin intervening septa. Diploetic – marrow spaces with few air cells. Sclerotic / Acellular : no cells or marrow spaces. Mastoid antrum is small & sigmoid sinus is anteposed. 49 drsurajmmch
- 50. 50 drsurajmmch
- 51. MASTOID AIR CELLS The mastoid air cells are traditionally divided into several groups, which include: 1. Zygomatic cells: In the root of zygoma. 2. Tegmen cells: Extending into the tegmen tympani. 3. Perisinus cells: Present over the sinus plate. 4. Retrofacial cells: Present round the fallopian canal of facial nerve. 5. Perilabyrinthine cells: They are located above, below and behind the labyrinth. The cells, which are present in the arch of superior semicircular canal, may communicate with the petrous apex. 6. Peritubal cells: They are present around the eustachian tube. These and the hypotympanic cells communicate with the petrous apex. 7. Tip cells: These large cells lie in the tip of mastoid medial and lateral to the digastric ridge. 8. Marginal cells: These cells, which lie behind the sinus plate, may extend into the occipital bone. 9. Squamous cells: They lie in the squamous part of temporal bone. 51 drsurajmmch
- 52. 52 drsurajmmch
- 53. MUCOUS MEMBRANE OF ME Mucous membrane of nasopharynx is continuous with middle ear, aditus, antrum & mastoid air cells. It wraps the structures of ME like peritoneum of abdomen, dividing the cavity into various compartments. Better to say all the structures are outside the mucous membrane. Eustachian tube : Cartilaginous part – pseudostratified columnar Bony part - columnar Tympanic cavity : Antero-inferior part – ciliated columnar Posterior part – cuboidal Epitympanum & mastoid air cells – non-ciliated, flat epithelium. 53 drsurajmmch
- 54. COMPARTMENTS OF ME Ossicles and their mucosal folds separate mesotympanum from epitympanum (attic). Compartments of Epitympanum 1. Prussak’s space: Its boundaries, which limit spread of infection to other compartments, are following: Lateral: Membrana flaccida (Shrapnell’s membrane) Medial: Neck of malleus Floor: Lateral process of malleus Roof: Fibers of lateral malleal ligament arising from neck of malleus and inserting along the rim of notch of Rivinus 54 drsurajmmch
- 55. 55 drsurajmmch
- 56. 56 drsurajmmch
- 57. COMPARTMENTS OF ME 2. Attic compartments: Transversely placed superior malleolar fold divides attic into two compartments – smaller anterior and larger posterior. The space between the lateral malleolar fold and lateral incudal fold provides communication with Prussak’s space. 2 compartments – Anterior attic compartment Posterior attic compartment: Superior incudal fold divides this space into following two divisions: Medial space Lateral space 57 drsurajmmch
- 58. 58 Postero-superior & lateral view of right tympanic cavity showing compartments & folds of ME drsurajmmch
- 59. COMPARTMENTS OF ME Compartments of Mesotympanum: In the upper part of mesotympanum there are following three compartments. 1. Inferior incudal space: Its boundaries are following Superior: Lateral incudal fold Medial: Medial incudal fold Lateral: Posterior malleolar fold extending from neck of malleus to posterosuperior margin of tympanic sulcus. Anterior: Interossicular fold that lies between long process of incus and upper two-third of handle of malleus. 59 drsurajmmch
- 60. COMPARTMENTS OF ME 2. Anterior pouch of von Troeltsch: It lies between the following boundaries: Medial: Anterior malleolar fold extending from neck of malleus to anterosuperior margin of tympanic sulcus Lateral: Portion of the tympanic membrane anterior to handle of malleus 3. Posterior pouch of von Troeltsch: It is situated between the following boundaries: Medial: Posterior malleolar fold extending from neck of malleus to posterosuperior margin of tympanic sulcus. Lateral: Portion of the tympanic membrane posterior to handle of malleus. 60 drsurajmmch
- 61. 61 drsurajmmch
- 62. 62 drsurajmmch
- 63. 63 drsurajmmch
- 64. 64 drsurajmmch
- 65. KORNER’S SEPTUM Mastoid develops from the squamous and petrous parts of temporal bone. In some cases petrosquamosal suture persists as a bony plate called Korner’s septum, which separates superficial squamosal cells from the deep petrosal cells. During the mastoid surgery, Korner’s septum causes difficulty in locating the antrum and the deeper cells. If not recognized, Korner’s septum leads to incomplete removal of disease during mastoidectomy. Mastoid antrum can be entered into only after the removal of Korner’s septum 65 drsurajmmch
- 66. 66 drsurajmmch
- 67. BLOOD SUPPLY Following branches of external and internal carotid arteries supply blood to middle ear: External Carotid Artery Maxillary artery Anterior tympanic artery: Major contributor Middle meningeal artery Petrosal branch Superior tympanic artery: It traverses along the canal for tensor tympanic muscle. Artery of pterygoid canal: Branch that runs along eustachian tube. Posterior auricular artery Stylomastoid artery: Major contributor Ascending pharyngeal artery Tympanic branch Internal Carotid Artery: petrous part • Caroticotympanic branches. 67 drsurajmmch
- 68. VENOUS DRAINAGE Veins from the middle ear cleft drain into pterygoid venous plexus, superior petrosal sinus and sigmoid sinus. LYMPHATIC DRAINAGE The lymphatics of middle ear drain into retropharyngeal and parotid nodes. Eustachian tube lymphatics drain into retropharyngeal group of lymph nodes . Internal ear does not have any lymphatics. 68 drsurajmmch
- 72. 72 drsurajmmch
- 73. UNDERSTAND THE ACTUAL VIEW (LEFT EAR) Left ear, 0° endoscope: View of the tympanic cavity after elevation of the tympano-meatal flap. The meso-and hypotympanum as well as parts of the epi-, retro-and protympanum are visualized. u: umbo m: manubrium sp: short process n: neck of the malleus pr: promontory jn: Jacobson nerve hy: hypotympanum fi: finiculus sst: sinus subtympanicus se: styloid eminence pe: pyramidal eminence st: stapedial tendon isj: incudostapedial joint fn: facial nerve ttm: tensor tympani muscle ttf: tensor tympani fold ica. Internal carotid artery drsurajmmch 73
- 74. Development of the middle ear is not covered in this presentation. If you are interested then please mail me. I will try to upload it as a separate one. 74 drsuraj1997@gmail.com
- 75. 75