


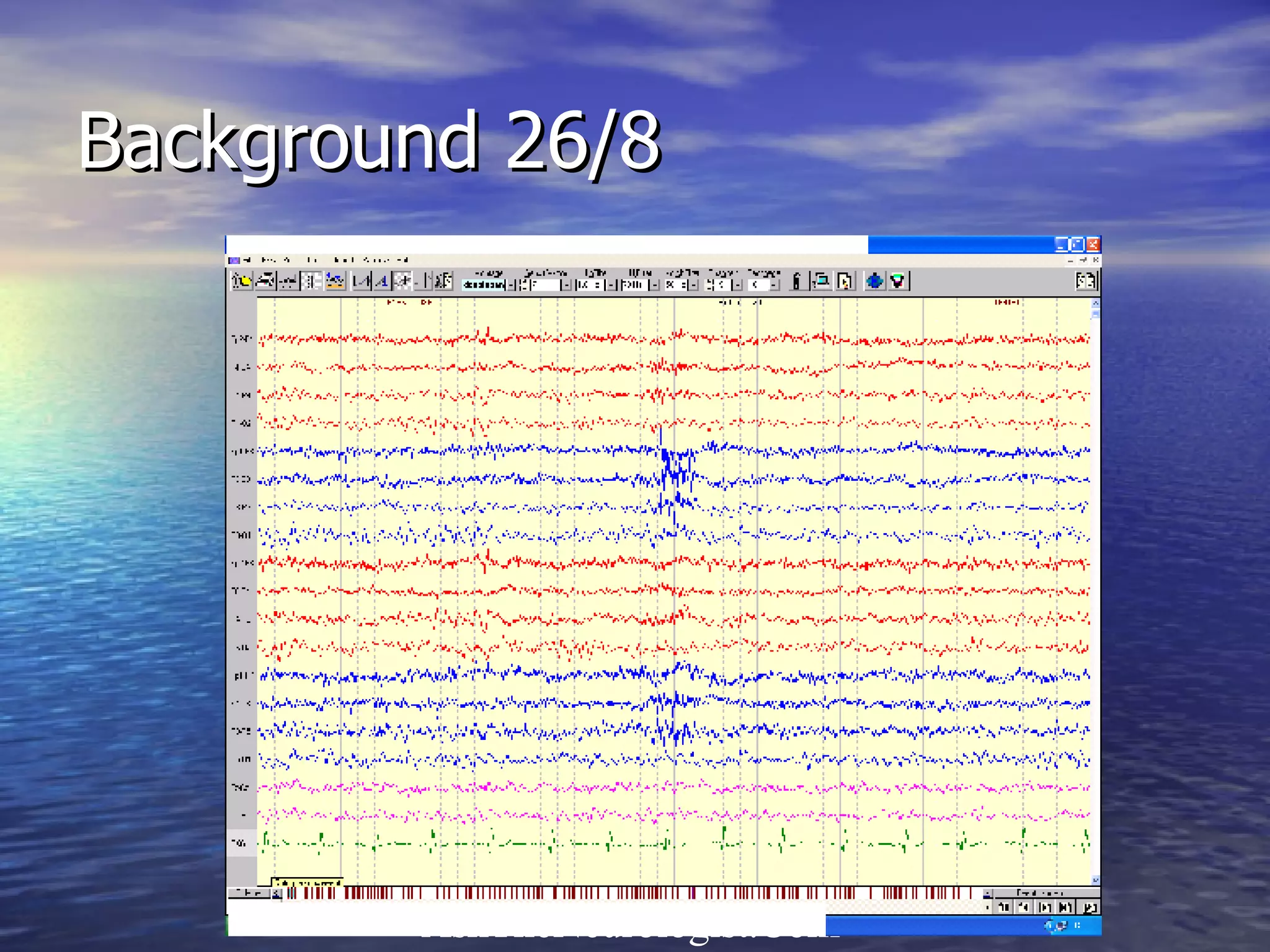


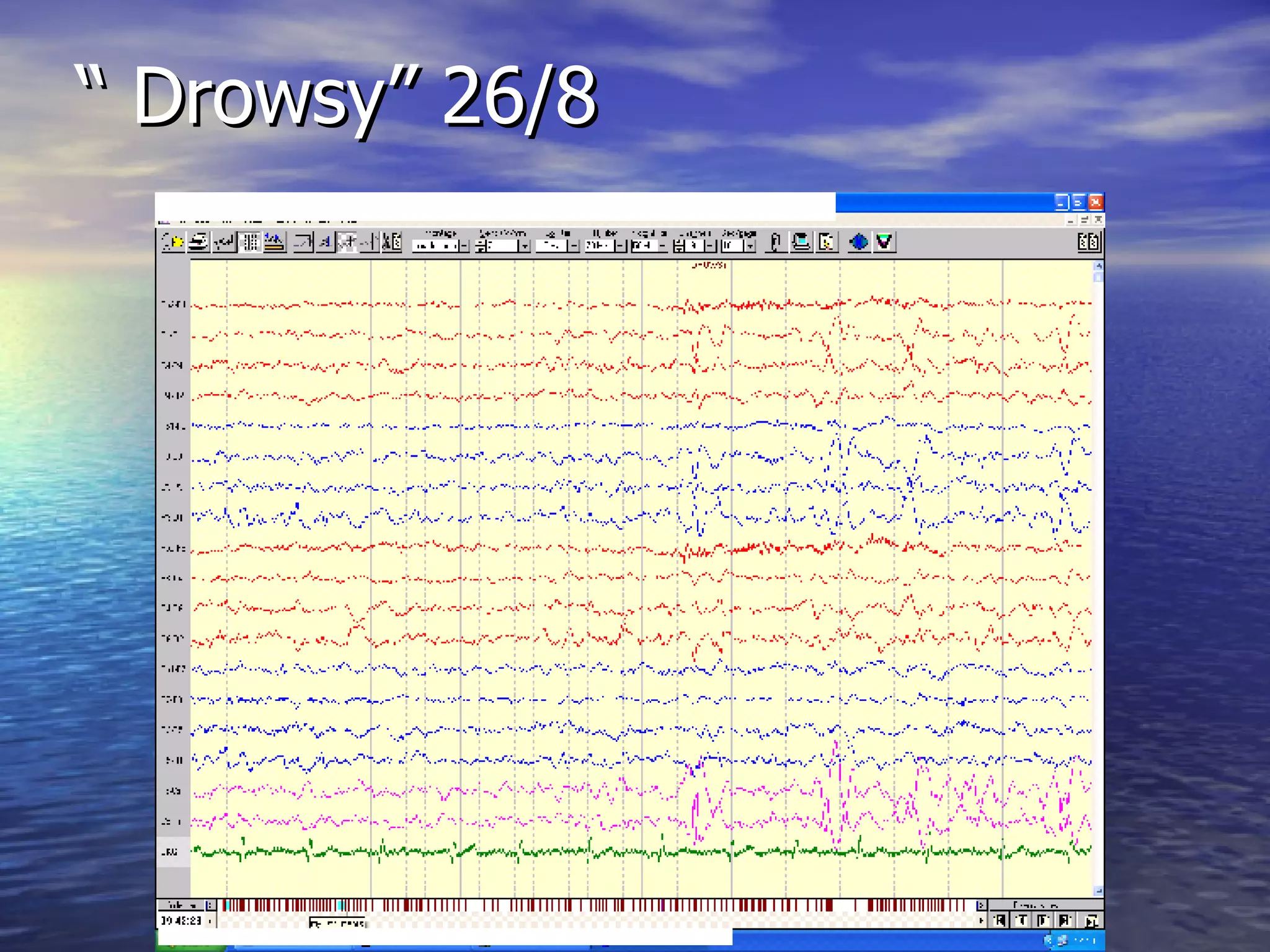

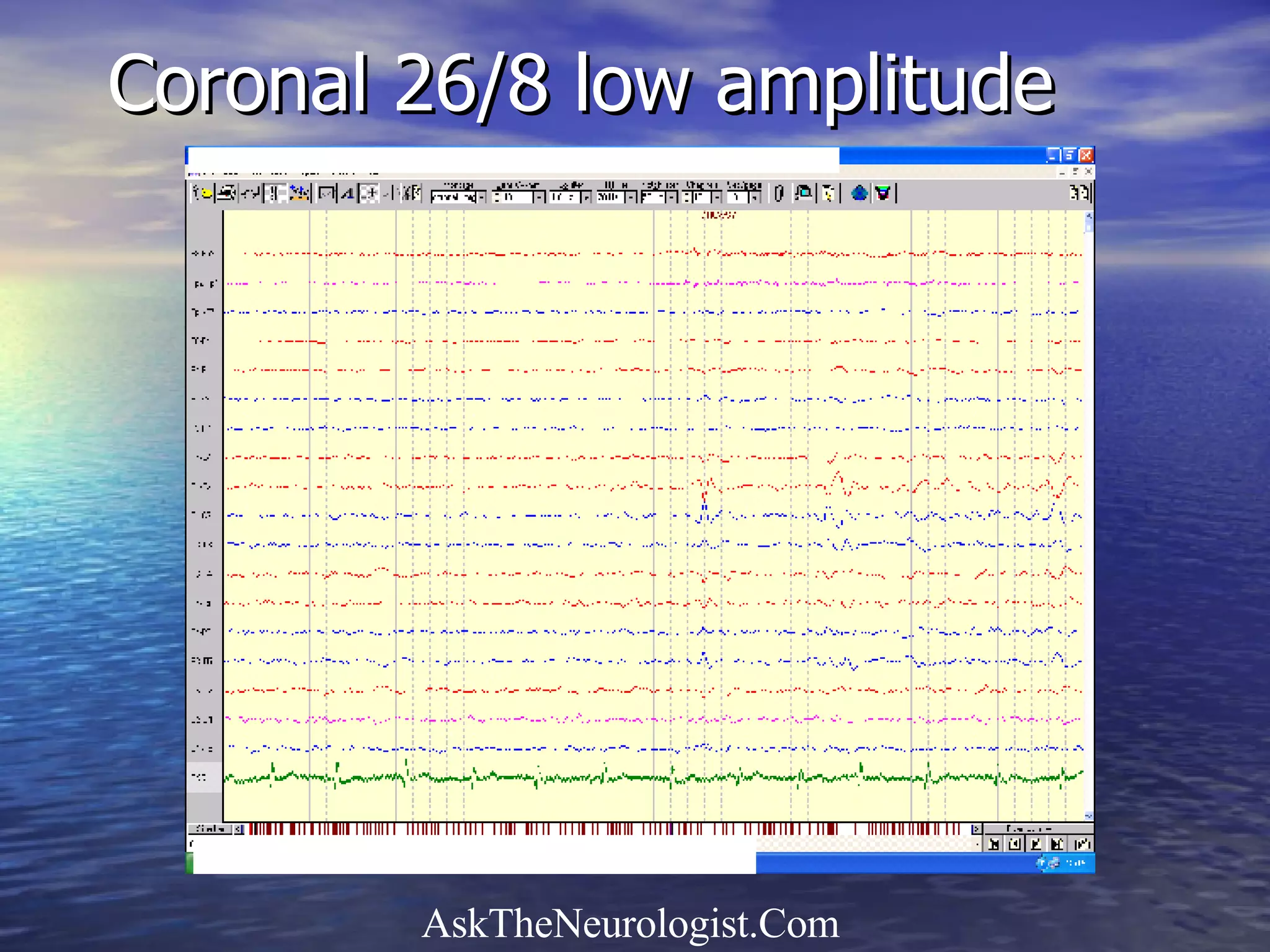


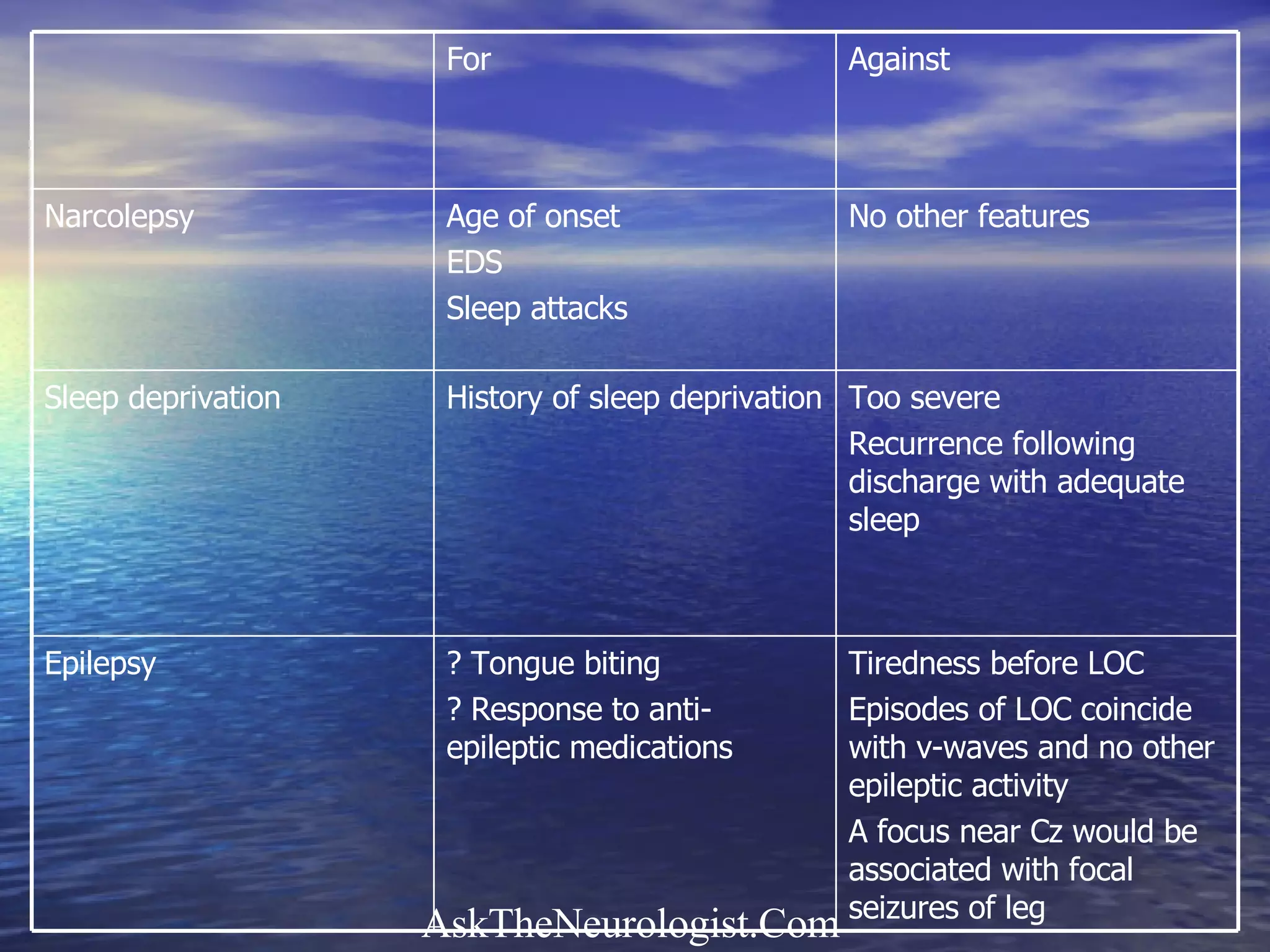














The document discusses a 16-year-old woman experiencing excessive daytime sleepiness, loss of consciousness, and tongue-biting, ultimately leading to consideration of narcolepsy versus epilepsy. Investigations included EEGs that revealed drowsy synchronous high amplitude activity, and the patient displayed significant improvements with anti-epileptic medications. The document also details narcolepsy symptoms, their potential causes, and associated conditions such as REM sleep behavior disorder and cataplexy.

![Narcolepsy[1]](https://cdn.slidesharecdn.com/ss_thumbnails/narcolepsy1-101115170759-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)









































































































