




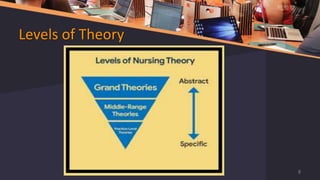































Prof. Dr. Chinna Chadayan.N discusses various conceptual frameworks and theories in nursing. Some key points discussed include: - The meaning and definitions of theories, concepts, models, and frameworks. - The three levels of nursing theory: grand, middle-range, and practice-level theories. - The nursing metaparadigm which includes person, environment, health, and nursing. - Several influential nursing theorists are discussed such as Nightingale, Peplau, Henderson, Abdellah, Orlando, Watson, Rogers, Orem, King, and their respective theories.