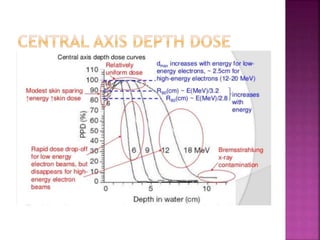
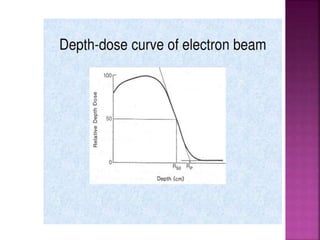
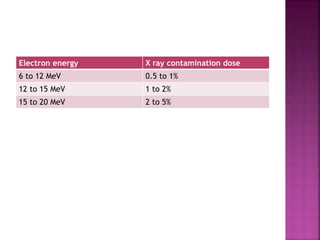
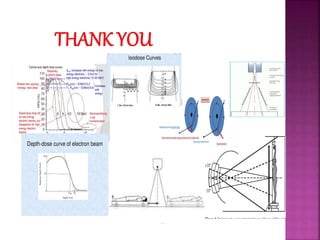
Electron beam radiotherapy uses megavoltage electron beams ranging from 6-20 MeV to treat superficial tumors within 6 cm of the skin surface. It provides a uniform dose at a specified depth with rapid dose fall-off, sparing deeper tissues. Common tumors treated include skin, lymphomas, and breast tissue. Electrons deposit dose via interactions with atomic electrons and nuclei, with dose decreasing rapidly beyond the 90% depth. Beam characteristics like central axis depth dose, isodose curves, and field size must be carefully considered for treatment planning.