
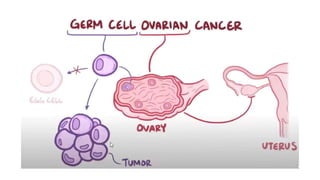
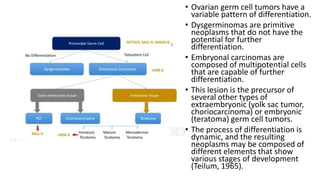

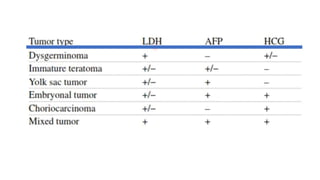

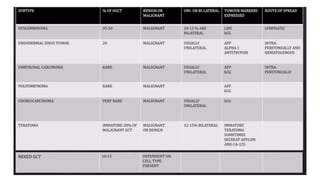
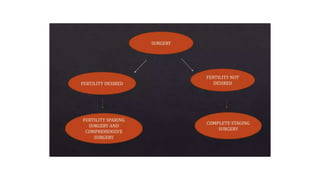
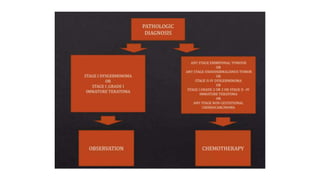
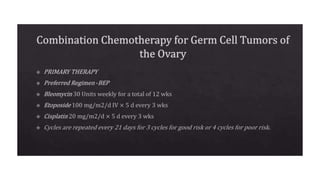


This document discusses germ cell tumors of the ovary. It begins by explaining that germ cell tumors originate from primordial germ cells and make up about 90-95% of ovarian malignancies in young women. It then covers the various subtypes of germ cell tumors, including their incidence rates, typical patient demographics, clinical presentations, diagnostic markers, pathological classifications, treatment approaches, and prognosis. Dysgerminoma is discussed as the most common subtype, while immature teratoma, endodermal sinus tumor, embryonal carcinoma, and choriocarcinoma are also described in terms of their defining characteristics and management. Throughout, the focus remains on applying knowledge from testicular germ cell tumor research























![Chapter 39 role of radiotherapy in benign diseases.pptx [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/chapter39roleofradiotherapyinbenigndiseases-191105205437-thumbnail.jpg?width=640&height=640&fit=bounds)










![Ovarian Cancer[1].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/ovariancancer1-240123055736-28b84740-thumbnail.jpg?width=640&height=640&fit=bounds)









![Ovarian tumour part-2 [Autosaved] [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/ovariantumourpart-2autosavedautosaved-230506134441-2d383801-thumbnail.jpg?width=640&height=640&fit=bounds)






























