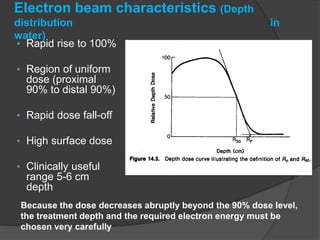
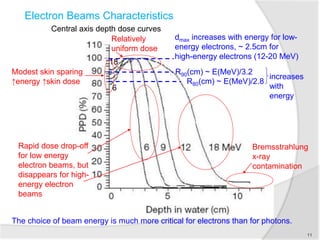
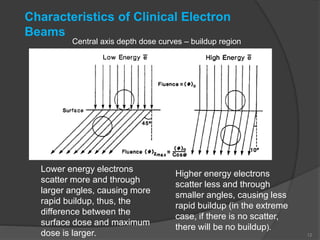
Electron beam therapy uses megavoltage electron beams to treat superficial tumors within 6 cm of the skin surface, sparing deeper tissues. The dose distribution of electron beams provides a uniform dose in the target region followed by a rapid dose fall-off. Treatment planning for electron beams requires consideration of electron energy, air gaps, tissue inhomogeneities, and adjacent fields to determine the optimal dose distribution. Electron beams can effectively treat many superficial cancers of the skin, limbs, and surgical beds.