Download to read offline



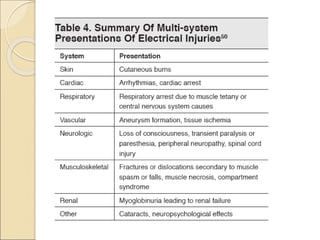
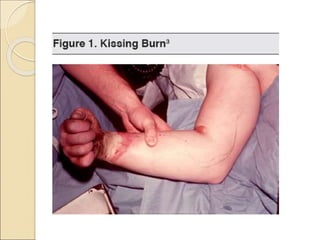
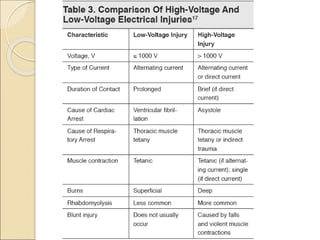
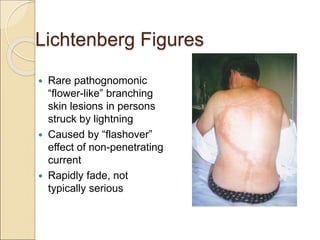
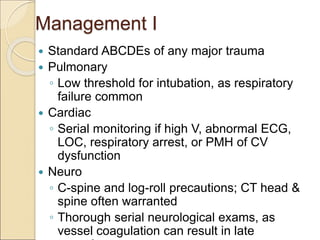



Electrical injuries account for around 3% of burn injuries and can be fatal. The extent of injury depends on factors like current, voltage, resistance, and duration of contact. High resistance tissues like bone are prone to deep burns while low resistance tissues conduct current. Direct effects can cause cardiac, neurological and respiratory issues. Thermal burns result from the conversion of current to heat. Management involves ABCs and monitoring for complications across organ systems like compartment syndrome and rhabdomyolysis. Prognosis depends on severity and development of multi-organ failure.









































![4N[sic] - Electrocution](https://cdn.slidesharecdn.com/ss_thumbnails/4nsic-electrocution-161227134451-thumbnail.jpg?width=640&height=640&fit=bounds)




![ELECTRICAL_AND_LIGHTNING[1] .6576875876587](https://cdn.slidesharecdn.com/ss_thumbnails/electricalandlightning1-250418104931-a1b02254-thumbnail.jpg?width=640&height=640&fit=bounds)
































