Downloaded 69 times









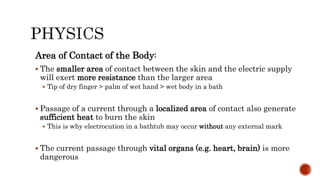






















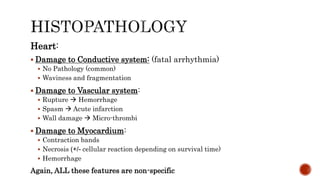






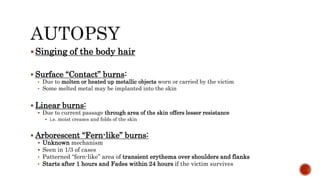




This document discusses electrical injuries and electrocution. It covers: - Types of voltages used in different countries and applications. - The differences between alternating and direct current. - Factors that determine the danger of electric currents, including amperage, voltage, duration of contact, resistance of tissues, and area of contact. - Common causes of death from electrocution like ventricular fibrillation or respiratory muscle spasm. - Characteristics of electrical injuries including entry and exit marks on the skin.









![[Forensics] traumatology 2.ppt](https://cdn.slidesharecdn.com/ss_thumbnails/forensicstraumatology2-150502144307-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)













![[Forensics] traumatology 1](https://cdn.slidesharecdn.com/ss_thumbnails/forensicstraumatology1-150502144040-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)







![ELECTRICAL_AND_LIGHTNING[1] .6576875876587](https://cdn.slidesharecdn.com/ss_thumbnails/electricalandlightning1-250418104931-a1b02254-thumbnail.jpg?width=640&height=640&fit=bounds)























































