Downloaded 49 times























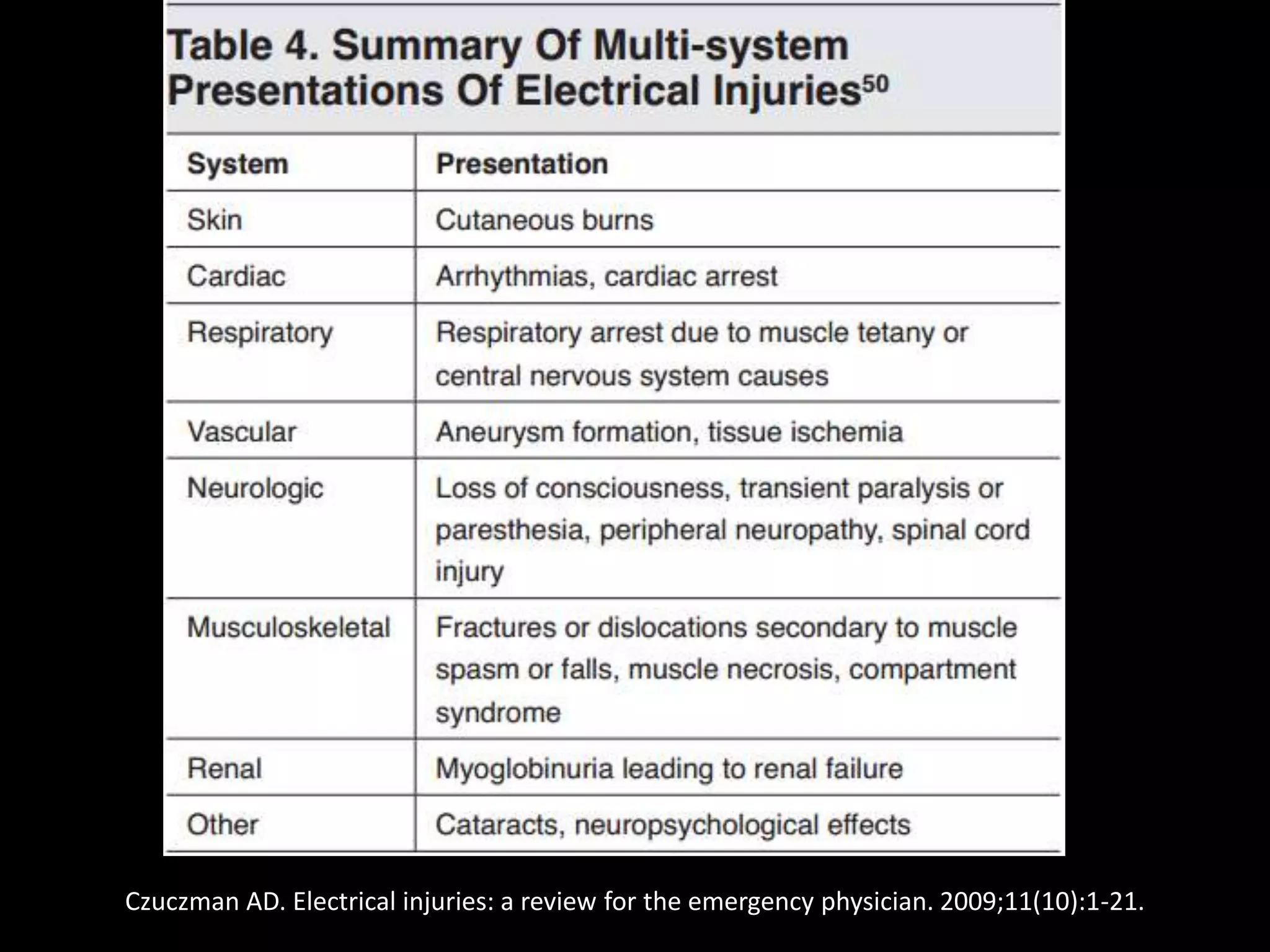




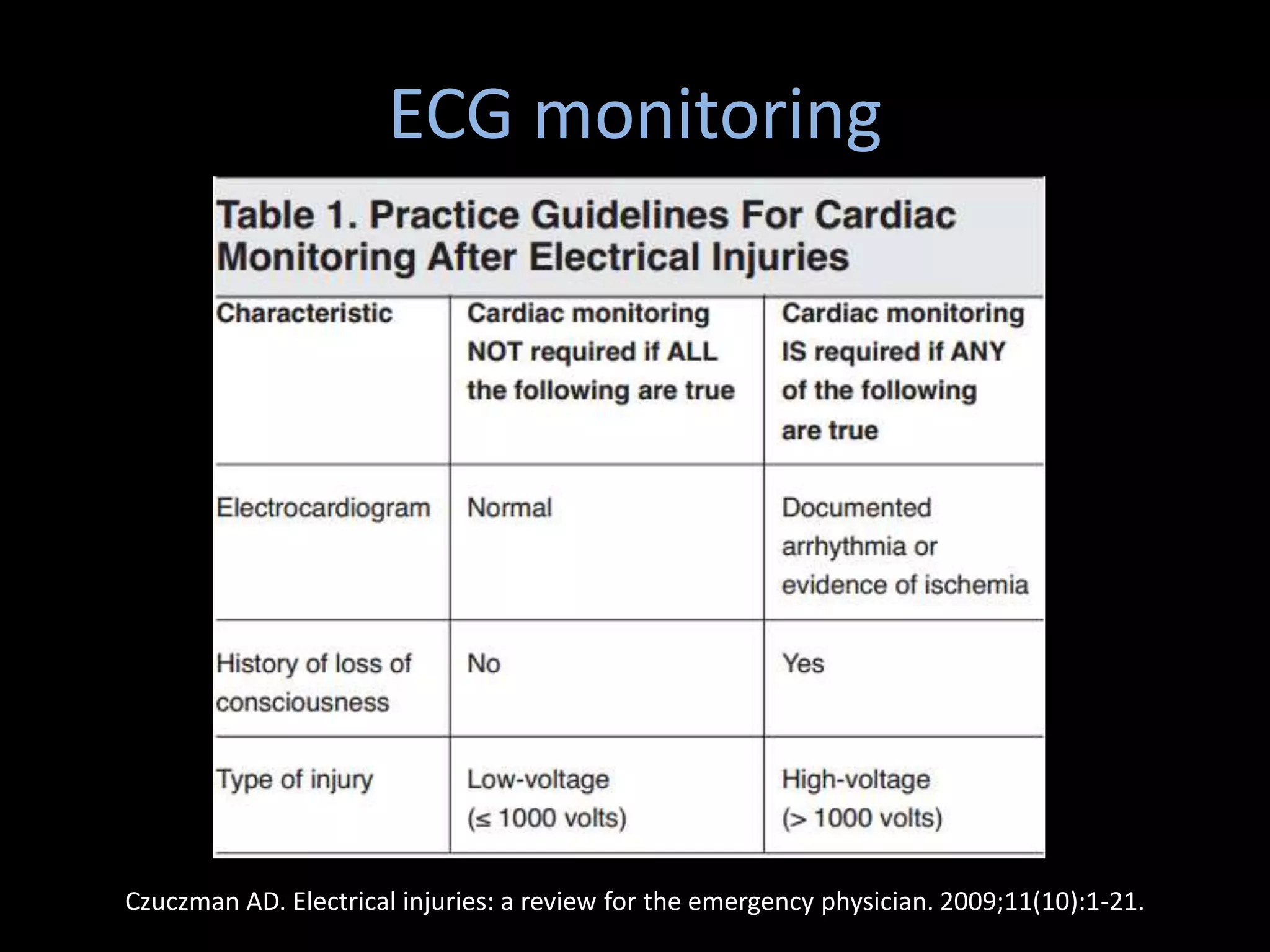








This document discusses electrical injuries, including the pathophysiology, mechanisms of injury, and treatment approaches. It notes that electrical injuries can cause severe burns, cardiac arrest, respiratory failure, muscle damage, and compartment syndrome. The severity depends on factors like voltage, current, resistance, and pathway of the electrical current. Treatment involves stabilizing the patient, monitoring for arrhythmias, treating burns, preventing compartment syndrome and renal failure, and managing pain. Wound care aims to remove dead tissue while preventing infection.























































































