Introduction
Burn injuriesare a world wide
problem. They rank high among
injuries suffered by man.
Since its inception in 1849, commercial
use of electricity has been one of the
most potentially dangerous
commodities in the world.
4.
Introduction
Electrical injuryincludes electrocution,
electric shock, burns and secondary
injuries.
The term electrical burn is used widely
to describe the variety of injuries
created by supraphysiologic electrical
energy interacting with living tissue.
5.
Epidemiology
According tostatistical data, 0.8-1% of
accidental deaths are caused by an
electric injury.
Electric injury accounts for 1000 deaths
each year in the United States, with a
mortality rate of 3-15%
6.
Epidemiology
Approximately 20%of all electrical injuries
occur in children, with a bimodal peak incidence
highest in toddlers and adolescents.
Most electrical injuries that occur in children are
at home, with extension cords (60-70%) and wall
outlets (10-15%) being by far the most common
sources in this age group.
Electrical burns account for 2-3% of all burns in
children that require emergency room care.
7.
Epidemiology
Electrical burnsconstituted 2.8% of total
burn admissions.
Male: Female ratio was 1.8:1
44.9% of the patients were children with
age range between 22 days – 14 years.
Department of Burns, Plastic & Reconstructive Surgery, National
Orthopaedic Hospital Enugu(Niger ian J Clin Pract. 2006 Dec;9(2):124-
7.)
8.
Aetiology
Electrical burnsare usually divided into low
voltage and high voltage injuries, the threshold
being 1000volts.
a) Low voltage injuries: do not have enough
energy to cause destruction to significant amt of
subcutaneous tissues. The entry and the exit
points, normally in the fingers and toes suffer
small deep burns.
b) High voltage injuries
9.
Pathophysiology
Electrical energycausing direct tissue
damage, altering cell membrane resting
potential, and eliciting muscle tetany.
Conversion of electrical energy to thermal
energy, causing massive tissue destruction
and coagulative necrosis.
Mechanical injury with direct trauma
resulting from falls or violent muscle
contraction.
10.
Pathophysiology
Factors thatdetermine the degree of injury
include
Type of current
Resistance encountered
Current pathway
Magnitude of energy delivered
Duration of contact.
11.
Type of current
The repetitive nature of AC increases the
likelihood of current delivery to the
myocardium, which can precipitate
ventricular fibrillation.
In contrast, DC usually causes a single
violent muscle contraction, often
thrusting the victim away from the
source.
12.
Resistance
In general,tissues with high fluid and
electrolyte content conduct electricity
better.
Bone is the tissue most resistant to the
flow of electricity.
Nerve tissue is the least resistant, and
together with blood vessels, muscles,
and mucous membranes offer a path of
low resistance for electricity.
13.
Resistance
Skin isthe most important factor
impeding current flow. It is the primary
resistor against electrical current, and its
degree of resistance is determined by its
thickness and moisture.
It varies from 1000 ohms for humid thin
skin to several thousand ohms for dry
calloused skin.
14.
Pathway
Transthoracic currentscan cause fatal
arrhythmia, direct cardiac damage, or
respiratory arrest.
Transcranial currents can cause direct
brain injury, seizure, respiratory arrest,
and paralysis.
15.
Magnitude
The currentintensity will also
determine the magnitude of injury.
There may be individual variation on
the energy dose for a specific effect.
Less energy is generally required in
children, who have more water content
and thin skin and, hence, better
conductivity and less resistance.
16.
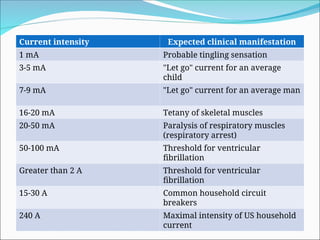
Current intensity Expectedclinical manifestation
1 mA Probable tingling sensation
3-5 mA "Let go" current for an average
child
7-9 mA "Let go" current for an average man
16-20 mA Tetany of skeletal muscles
20-50 mA Paralysis of respiratory muscles
(respiratory arrest)
50-100 mA Threshold for ventricular
fibrillation
Greater than 2 A Threshold for ventricular
fibrillation
15-30 A Common household circuit
breakers
240 A Maximal intensity of US household
current
Management
Acute emergency,shout for help.
Secure yourself.
Separate the victim from the current's source.
The safest way to do so is to shut off the current
e.g by throwing a circuit breaker or switch or by
disconnecting the device from an electrical
outlet.
Treat as multi-trauma patient with cervical
immobilisation at least until the full extent of
injuries has been quantified
Complications
Seizures
Peripheralnerve damage
Psychiatric problems from depression to
aggressive behaviour
Cataracts
Paraplegia/Quadriplegia
Deformities
25.
Prevention
Education aboutand respect for electricity are
essential.
Ensure electrical devices are properly designed,
installed, and maintained.
Electrical wiring should be installed and serviced
by properly trained personnel.
Outlet guards reduce risk in homes with infants
or young children.
26.
PREVENTION CONTD.
Anyelectrical device that touches or may be
touched by the body should be properly
grounded.
Three-pronged outlets are safest.
Circuit breakers that interrupt (trip) circuits
when current as low as 5 milliamperes leaks are
advisable in areas that get wet, such as kitchens
and bathrooms and outdoors.
27.
CONCLUSION
Although electricalburns represent only a small
proportion of burn injuries, the incidence of
complications, mortality and morbidity, and
disability is high. Such injuries can be prevented
with proper educational programmes designed
to suit the community.










































![4N[sic] - Electrocution](https://cdn.slidesharecdn.com/ss_thumbnails/4nsic-electrocution-161227134451-thumbnail.jpg?width=640&height=640&fit=bounds)



























